Behavioral Health Payer Contracting: A Practice Owner's Guide
Behavioral health payer contracting is a negotiation, not a form. Learn how to read a payer contract, benchmark your rate, and negotiate a better one.


Cameron Fletcher
Head of Growth at PayerPrice
You left a group practice to start your own. To keep the clients who followed you, you needed to get in-network fast, so you signed the payer contracts as they arrived. The paperwork was dense, the rate was buried in a formula you did not fully decode, and getting paneled felt more urgent than reading the fine print.
Months later you find out what you actually signed. Jeremy Hinote, a licensed professional counselor who owns a practice in Augusta, Georgia, described the moment on the Wise Practice Podcast. He had agreed to a percentage of a number he never saw clearly.
"What I had signed was to take a percentage of this other amount that was really low and actually was my lowest reimbursement. A friend of mine who is not fully credentialed with Tricare, is not fully in network, and her reimbursement is higher than mine. She's just a few miles from me."
- Jeremy Hinote, LPC, owner of Savannah River Counseling
The rate is only the first cost. Dr. Jen Blanchette, a psychologist who ran an insurance-based practice, went five months without payment from a single insurer during the pandemic. Dr. Jeremy Sharp, who owns a 20-clinician assessment group, spent eight months and more than 30 phone calls chasing nearly $100,000 in unpaid claims caused by one payer loading his contract wrong. A bad contract does not just pay less. It costs you in denied claims, clawbacks, and the hours you spend fighting for money you already earned.
This guide is the part the rest of the internet skips. You will learn how to read a payer contract before you sign it, how to find out whether your rate sits below market, the negotiation moves that took one owner from a 2 percent offer to 20 dollars more per session, and how to choose which payers are worth taking at all. Behavioral health payer contracting is a negotiation, not a form you fill out, and you have more leverage than you think.
Contracting versus credentialing: why being credentialed does not mean getting paid
Credentialing verifies your qualifications, contracting is the business agreement that sets your rate and terms, and being credentialed without a signed contract means your claims get denied. Owners conflate the two constantly, and the confusion costs them money when they start billing against a contract that does not exist yet.
Credentialing is the payer's vetting process. It confirms your license, your malpractice coverage, your education, and your work history, usually through your CAQH profile. Contracting is the separate step where the payer offers you a participation agreement: the fee schedule, the clauses, and the effective date. Licensing is a third thing entirely, granted by your state board, not the payer. According to Pimsy EHR, credentialing alone runs 90 to 180 days per panel, and a provider who is credentialed but not contracted sits in a limbo where claims bounce back unpaid.
The effective date is where owners lose real revenue. You cannot bill for sessions delivered before your contract loads, so every week you see in-network patients ahead of that date is a week you eat the cost. The contract, not the credentialing approval, is the document that decides your income. That is why you read it before you sign it.
Read the contract before you sign: what to check
Before you sign, check three things: how the rate is calculated, what each CPT code pays, and the clauses that quietly drain money after the ink dries. Most owners check none of them because getting paneled feels urgent and the contract looks standard. It is not standard, and the differences are worth thousands of dollars a year.
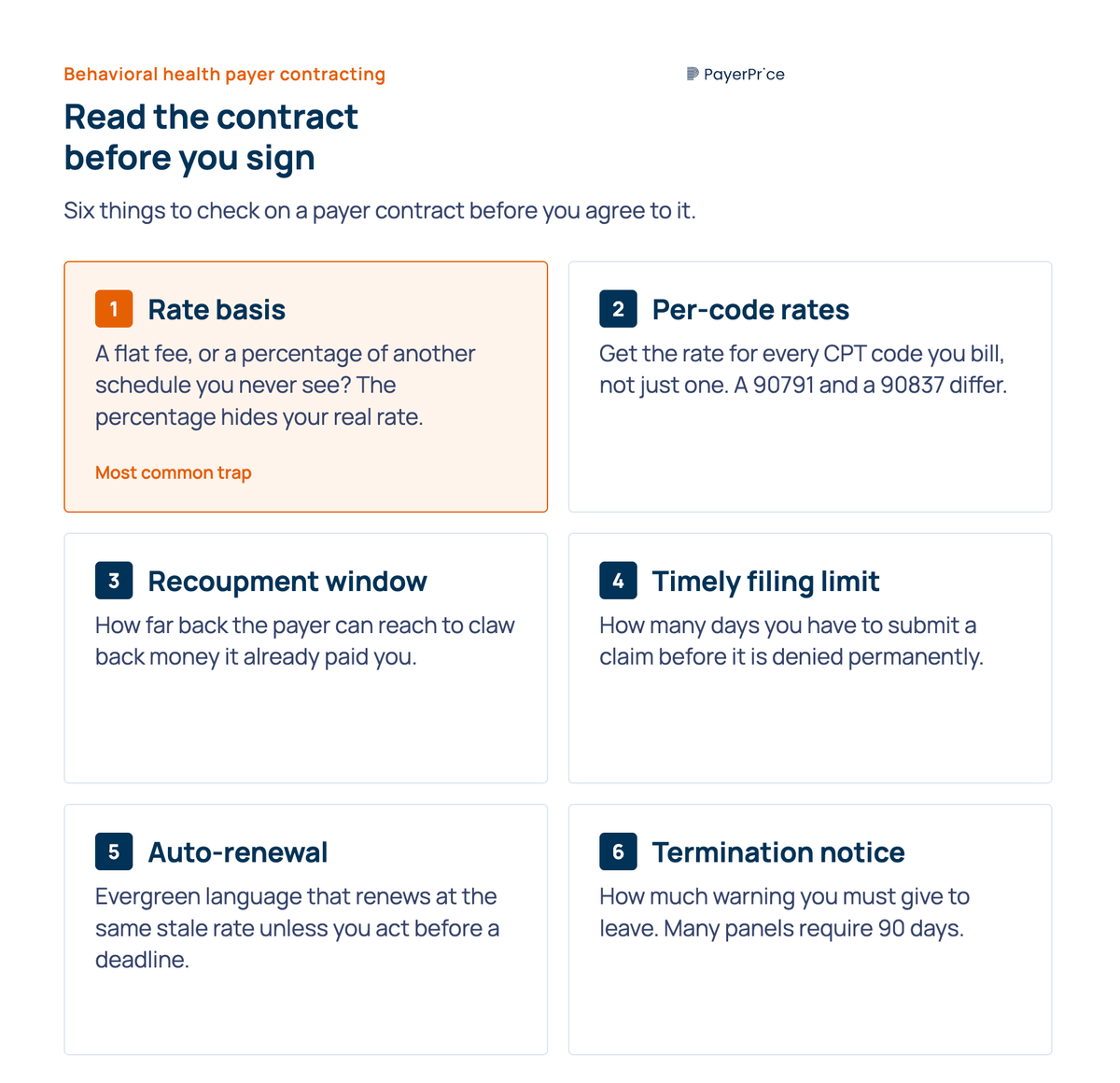
Start with the rate basis. Some contracts list a flat dollar amount per code. Others pay a percentage of a separate fee schedule you never see, which is exactly the structure that gave Hinote his lowest rate. If a contract pays "a percentage" of anything, ask for the underlying schedule in writing and calculate the actual dollar figure per code before you agree to it.
Next, check the rate for every code you bill, not just one. A diagnostic evaluation (90791), a 60-minute session (90837), and a 45-minute session (90834) are priced differently, and a contract that looks fine on one code can underpay badly on another. Ask for the full fee schedule covering each CPT code your practice uses.
Then read the clauses that cost money later. Look for these specifically:
- Recoupment, or clawback, windows: how far back the payer can reach to take back money it already paid you.
- Timely filing limits: how many days you have to submit a claim before it is denied permanently.
- Auto-renewal, or evergreen, terms: language that renews your contract at the same stale rate unless you act before a deadline.
- Termination notice: how much warning you must give to leave. Many panels require 90 days.
Reading the contract tells you what you are being offered. It does not tell you whether that offer is good. For that, you need a number to compare it against.
Know your number: is your rate below market?
Your contracted rate is below market when it falls under what comparable behavioral health providers in your region collect for the same CPT code, and you find that number before you negotiate, not after. The single most common reason owners accept a low rate is that they have no idea what a fair one looks like.
Market rate is not one number. It varies by CPT code, by region, by license level, and by payer. A 90837 in a metro area with a provider shortage commands more than the same code in a saturated suburb. The rate a doctoral psychologist negotiates differs from a master's-level clinician's. Your job is to find the realistic range for your codes, your license, and your geography.

You have several ways to find that range:
- Peer networks. Other owners in your area know what they collect, and many will share ranges if you ask directly.
- Medicare as a floor. The Medicare fee schedule is public and gives you a reference point that most commercial rates sit above.
- State Medicaid rates. Published and useful for understanding the bottom of your market.
- Benchmarking tools. Services like PayerPrice aggregate contracted rates so you can compare your offer against what others actually collect, by code and region.
For code-level Medicare and commercial reference rates across the full behavioral health code set, the PayerPrice behavioral health coding guide breaks down what each code pays. Use it as your reference point, then use this article to act on the gap.
The gap between a good rate and a bad one is large enough to decide whether a panel is worth keeping. Sharp found that his two lowest-paying panels paid 25 to 30 percent less than his highest, for the same work. Once you know where your rate sits against the market, you stop guessing and start negotiating from a position you can defend.
The negotiation playbook: how to get a payer to raise your rate
To raise your rate, request the increase in writing with your benchmark data attached, use the leverage you actually hold, and plan for several rounds rather than one. The first thing to internalize is that most owners never ask. As Hinote put it, the majority do not realize asking is an option.
"I think there's a majority of people that don't even realize you can actually go to the insurance panel that you're signed on with and contracted with and ask for raises along the way."
- Jeremy Hinote, LPC, owner of Savannah River Counseling
The mindset prerequisite is a willingness to walk away. A payer that knows you will sign anything has no reason to move. Hinote had to reach the point where leaving was a real option for him, even though the panel represented 40 to 50 percent of his caseload, before he pushed hard. You do not have to leave. You have to be genuinely prepared to.
Your leverage is more concrete than it feels. Use whichever of these applies to you:
- Network adequacy gaps. If the payer is short on providers in your area, it needs you more than it lets on, and a closed-panel denial often reverses when you point this out.
- A specialty or population. Eating disorders, substance use, autism assessment, or a specific language or community you serve all raise your value to a payer trying to meet coverage requirements.
- An out-of-network position. If patients already see you out-of-network and the payer is paying out-of-network rates, you can argue an in-network contract saves them money.
- Multi-clinician volume. A group brings a roster, not one provider, and that volume is a negotiating chip a solo clinician does not have.
Set your expectations for the back-and-forth. The first offer is usually a token. Hinote's opening raise was around 2 percent, roughly two dollars more per session. He pushed back across four rounds over about two months and ended with close to 20 dollars more per session. The difference between the first offer and the final one came entirely from refusing to accept the first offer.
Timing matters for existing contracts. Request raises before an auto-renewal or anniversary date, when the payer faces the prospect of you reopening the agreement anyway. Tie the request to your benchmark data and the codes where you are furthest below market.
Negotiation fixes one contract at a time. The larger decision is which payers belong in your business at all.
No results
Adjust your filters or try a different code.
Build your payer mix: choose which payers to contract with
Not every payer is worth taking, and you evaluate each one on rate, payment reliability, and referral volume before you sign. Owners assume more panels mean more income. Past a point, the opposite is true.
The trap is over-paneling with low payers. Once you accept a low-reimbursing panel, the patients it sends become a growing share of your caseload, and you cannot easily replace them with better-paying ones. Hinote described exactly this risk.
"The trap you could get into is if you allow for too many of those low paying reimbursing insurance companies. Well now, all the people coming to your practice may only take those, and that may put you in a financial burden."
- Jeremy Hinote, LPC, owner of Savannah River Counseling
Rate is not the only cost. Sharp found that his lowest-paying panels were also the most labor-intensive, generating the most denials and billing work. A panel that pays less and costs more to administer loses money twice. Steve Priest, CEO of the addiction-treatment provider Spero Health, described the broader squeeze in Behavioral Health Business, where rate compression has tightened over recent years.
Sort every payer into one of three buckets:
- Take: pays at or above market, pays reliably, sends volume you want.
- Negotiate first: sends good volume but pays below market, so you contract only after pushing the rate.
- Decline: pays poorly and creates administrative drag with no offsetting referral value.
The point is to build a mix where your best payers carry your caseload, not your worst. Knowing what each payer is worth, before you sign, is what makes that possible.
Your first move this week
Behavioral health payer contracting rewards the owners who treat the rate as negotiable and punishes the ones who treat the contract as a form. Every owner quoted here learned the same lesson the expensive way: the offer in front of you is a starting point, and the gap between accepting it and negotiating it is measured in tens of thousands of dollars a year.
Start with one concrete step. Pull the contracts for your top three payers this week, find the rate each one pays for your most-billed code, and compare those rates against the market before you renew or sign anything else. The owners who know their number negotiate from data. The ones who do not get the lowest reimbursement on the panel and never find out.
Share this article
Help spread the knowledge by sharing with others
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Related Articles
Continue exploring healthcare transparency and compliance topics
Multi-Specialty Coding Guide: Billing in Multi-Specialty Practices
A multi-specialty coding and billing guide for physician groups. Covers CPT, modifier 25, NPP rules, and fee schedules in multi-specialty practices.
Healthcare Underpayments: A Provider's Recovery Guide
Healthcare underpayments hide as zero-balance claims no worklist ever flags. See how providers detect, recover, and prevent the revenue payers quietly keep.
Transparency in coverage data: how providers turn the payers' own files into negotiating leverage
The Transparency in Coverage rule was marketed as a consumer shopping tool, but the files it produced let provider contracting teams see what payers pay their competitors. This guide explains what's actually in the data, why the raw files mislead you, and how to use them to benchmark your rates and strengthen your next negotiation.