Healthcare Underpayments: A Provider's Recovery Guide
Healthcare underpayments hide as zero-balance claims no worklist ever flags. See how providers detect, recover, and prevent the revenue payers quietly keep.


Cameron Fletcher
Head of Growth at PayerPrice
Your payer sends a payment. Your billing system posts it. The claim closes at zero balance. Everyone moves on.
A zero balance does not mean the payer paid you correctly. It means your system reconciled what arrived against what the payer reported as allowed. If the payer applied an old fee schedule, downgraded a DRG, bundled two procedures that should have paid separately, or downcoded an office visit, the shortfall vanishes into a contractual adjustment that no one audits.
That is what makes underpayments different from denials. A denial is loud. It generates a code, lands in a worklist, and someone works it. An underpayment is silent. As Ned Lutz, founder of CoverageUnlocked, describes it:
"Downcoding is silent. The remit just comes back a little light. No denial document hits your queue. You can't appeal a haircut you never flagged, and most billing workflows have no trigger for 'paid, but paid wrong.'"
- Ned Lutz, founder, CoverageUnlocked
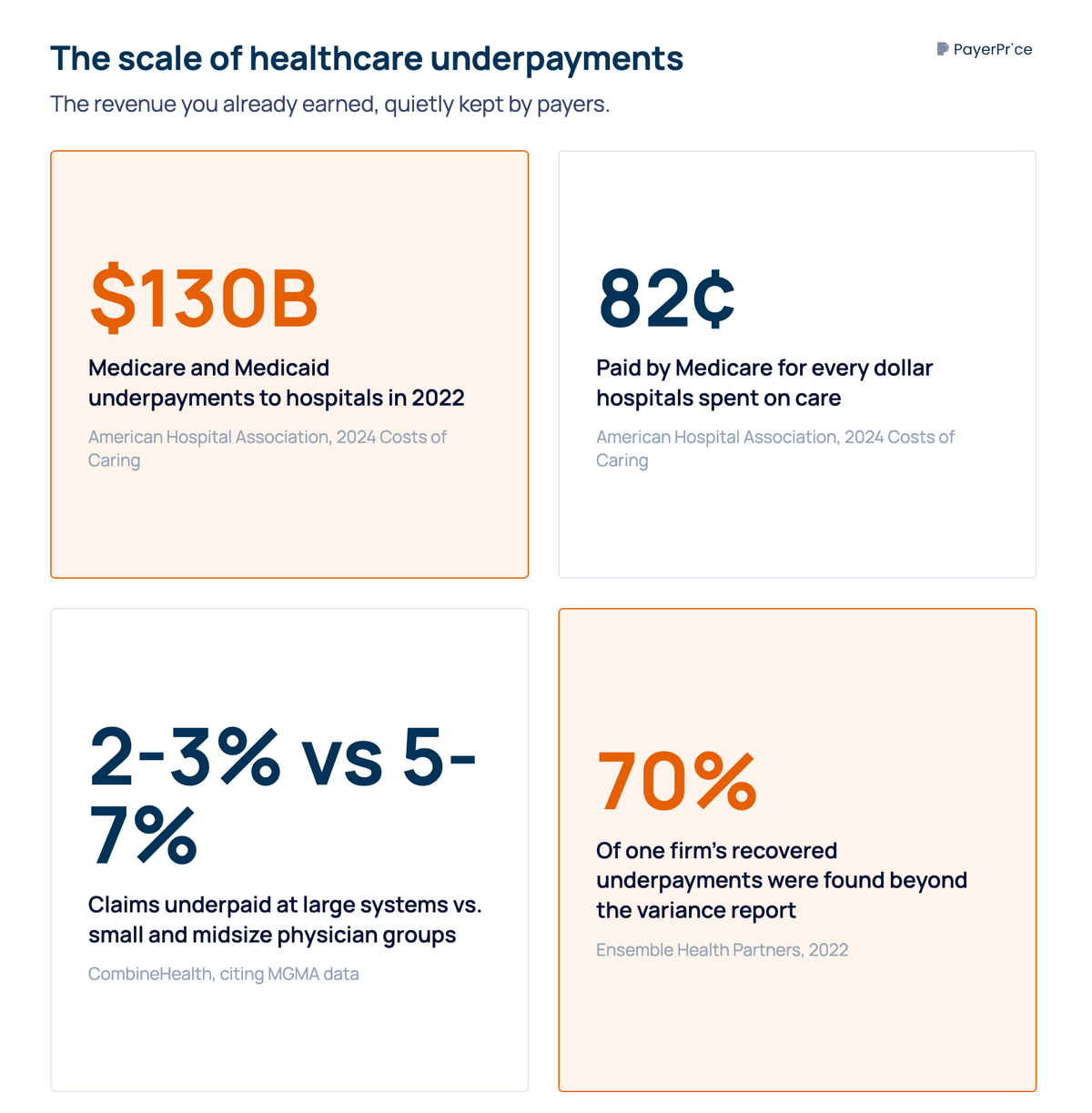
The money adds up fast. According to the American Hospital Association, Medicare and Medicaid underpayments totaled nearly $130 billion in 2022, and Medicare paid just 82 cents for every dollar hospitals spent on care. Commercial underpayments stack on top of that. This guide shows revenue cycle teams at hospitals, health systems, and physician groups how to find underpayments your variance report misses, recover them with an appeal payers cannot dismiss, and stop them from recurring.
What healthcare underpayments are (and why they aren't denials)
A healthcare underpayment occurs when a payer reimburses you less than the contracted or expected amount for a valid service you already delivered. The claim is not rejected. It is paid, just paid short.
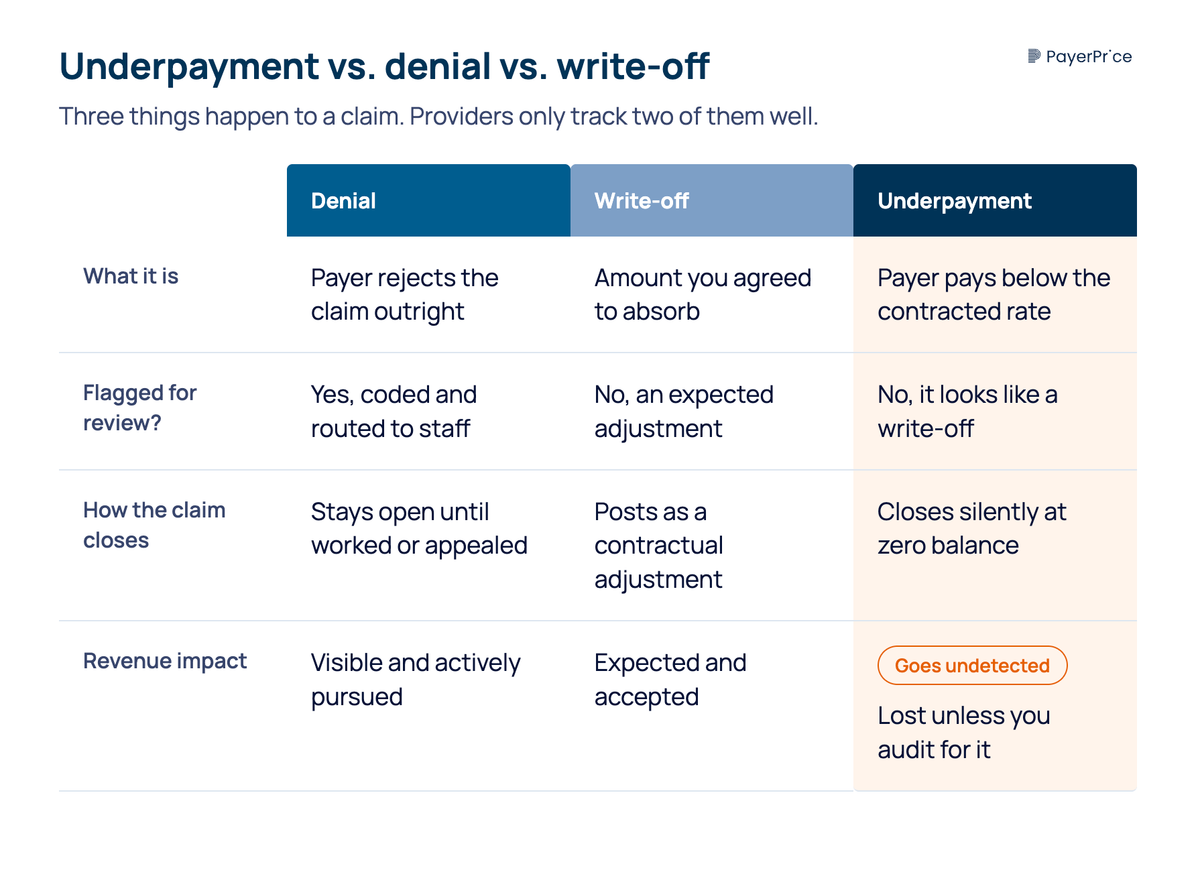
Three things happen to a submitted claim, and providers track only two of them well:
- A denial rejects the claim outright. It is visible, coded, and routed to staff who appeal it.
- A write-off is an amount you agreed to absorb, like a contractual adjustment you expected.
- An underpayment looks like a write-off but is not one. The payer recorded an allowed amount below your contract, and the difference was written off as if it were legitimate.
The operational problem is that underpayments hide inside that third bucket. Your denial dashboard never shows them. Your clearinghouse never rejects them. The claim posts, the system books the shortfall as a contractual adjustment, and the account closes. Nothing flags it for review.
The scale depends on your organization. According to CombineHealth, citing MGMA data, large health systems see 2% to 3% of claims underpaid, while small-to-midsize physician groups see 5% to 7%. On a $50 million book of revenue, 3% is $1.5 million in earned money a payer kept. Over five years, that compounds past $7 million.
Knowing underpayments exist is one thing. Understanding why they stay hidden tells your team where to look.
Why healthcare underpayments stay invisible
Underpayments stay invisible because they close as zero-balance accounts, and a zero balance signals "done" to every system and person downstream. No alert fires when a payment is short. The alert only fires when a payment is missing.
Consider a single claim. Your group bills CPT 99215 for an established patient visit. Your contract with Payer X allows $185. Payer X remits $162, your system posts the payment, writes off $23, and closes the claim. No flag. No notification. The same pattern repeats at the facility level when a payer disputes a DRG assignment and pays the lower-weighted group, or applies a stop-loss provision incorrectly on a high-dollar inpatient stay.
What makes this harder is that payers increasingly reduce payment without changing the billed code. The visit was coded 99215, billed 99215, and paid at the 99214 rate, with nothing in the remit announcing the change. Tom Buckley, senior vice president of revenue cycle and managed care at Virtua Health, has a name for it:
"We use the phrase here at Virtua, 'payer shenanigans.' The payer will come back and disagree with the DRG assignment, and we'll have to go through a lengthy exercise to defend our DRG assignment. They'll downgrade the E&M code, which, in essence, is paying you less."
- Tom Buckley, SVP of revenue cycle and managed care, Virtua Health
This behavior is now routine. According to the American Medical Association, payers are increasingly implementing E/M downcoding programs that inappropriately reduce payment for claims, and they do so in ways that make the reductions extremely difficult to identify in coding audits.
Most teams rely on a payment variance report to catch this, and the report only catches part of it. A variance report compares a payment against a stored expected rate, so it surfaces stop-loss, carve-out, escalator, and bundling variances. It misses underpayments that come from misapplied edits, alternate revenue-code logic, or rates that were never loaded correctly in the first place. According to Ensemble Health Partners, the firm recovered more than $200 million in underpayments for clients in 2022, and 70% of that was identified beyond the variance report. Treating the variance report as your full safety net leaves most of the leak uncaught.
If the report misses most underpayments, you need to know the specific payer and provider behaviors that create them.
What causes healthcare underpayments
Healthcare underpayments come from two sources: payer-side adjudication behavior and provider-side billing gaps. Splitting them this way tells you which problems to dispute and which to fix internally.
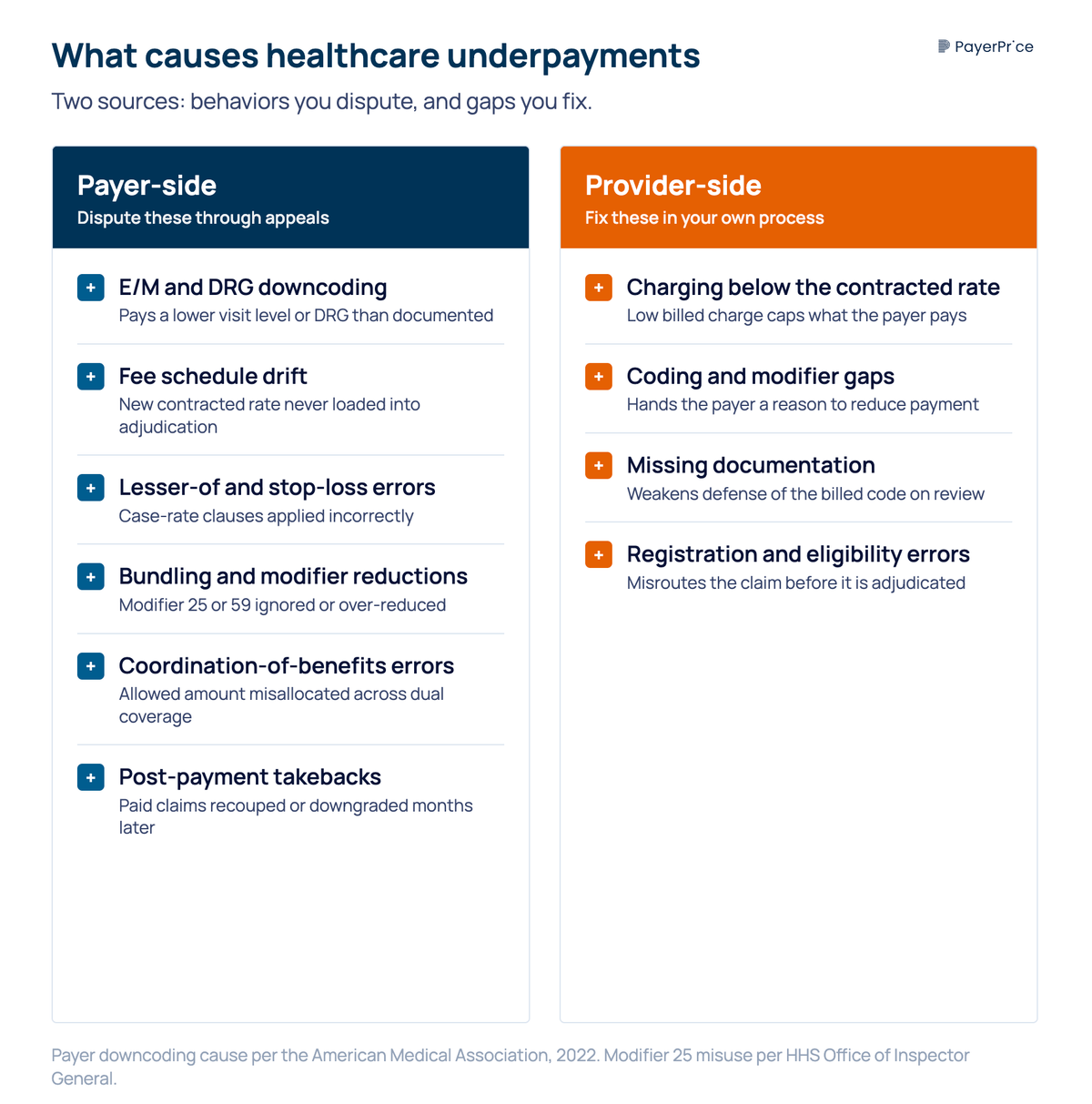
Payer-side causes generate the underpayments you recover through appeals:
- E/M and DRG downcoding. The payer pays a lower visit level or a lower-weighted DRG than documented and billed.
- Fee schedule drift. Your contracted rate increased at renewal, but the payer's system still adjudicates at the old rate. This is common on auto-renewed contracts where the new rate took effect on paper but was never loaded.
- Lesser-of and stop-loss errors. The payer applies a lesser-of clause or a stop-loss threshold incorrectly, paying billed charges or a percentage instead of the contracted case rate.
- Bundling and modifier reductions. The payer ignores modifier 25 or 59, or applies multiple-procedure reductions deeper than the contract allows. According to the HHS Office of Inspector General, 35% of Medicare claims using modifier 25 did not meet program requirements, and payers use findings like this to justify blanket reductions.
- Coordination-of-benefits errors. For patients with dual coverage, the primary payer shifts more of the allowed amount to the secondary payer or patient than the contract permits.
- Post-payment takebacks. A payer or its third-party vendor recoups or downgrades a claim months after it paid, often through a record review the provider cannot easily contest.
Provider-side causes generate underpayments you prevent by fixing your own process. These include charging below your contracted rate so the payer pays your low billed charge, coding or modifier gaps that hand the payer a reason to reduce payment, missing documentation, and registration or eligibility errors that misroute the claim.
The payer-side causes carry a deliberate edge, because the reductions are easiest to apply where the provider is least equipped to fight back. A biller at ENT Medical Services described the pattern on the AAPC forum:
"They are preying on offices not having enough time and staff to appeal these and just accepting what they pay. I appeal all of them with the office note attached. If you don't appeal anything they will just keep doing it."
- Biller, ENT Medical Services, AAPC billing forum
That dynamic scales from a small practice to a large system, and it points to the real work. Catching underpayments is only useful if you recover them.
How to detect and recover healthcare underpayments
Recovering an underpayment takes a repeatable process: detect the variance, build the appeal, and file it before the deadline closes. Each step has a concrete output, and the deadline is the part most teams underestimate.
Detection starts by going past the variance report. Build an expected reimbursement for every high-volume code and case rate, payer by payer, then compare it against what actually paid. Flag any claim where the payment falls below the expected amount, not just the claims your variance report already knows to question. Sort the flagged claims by code and payer so patterns surface. One claim paid short is a processing error. The same code paid short across hundreds of claims from one payer is a systematic underpayment, and systematic underpayments hold the recoverable revenue.
Once you have flagged claims, the appeal is what converts them to cash. A dismissible appeal asserts the payer paid wrong. A winning appeal proves it. Attach the following to every underpayment appeal:
- The contract language that sets the rate, with the relevant fee schedule line or case rate highlighted.
- The remittance advice showing what the payer actually paid.
- The corrected calculation, stating the contracted amount, the amount paid, and the exact difference owed.
- The clinical documentation that supports the billed code, for downcoding and DRG disputes specifically.
- The pattern evidence, when you are appealing a systematic underpayment, showing the same error across a batch of claims. A dispute covering 200 claims with one shared pattern is harder for a payer to wave away than 200 separate letters.
The deadline decides whether any of that matters. Build an appeal before the payer's filing window closes, because an underpayment you identify too late is permanently unrecoverable. Most commercial payer contracts allow 90 to 120 days from the date of payment to dispute, Medicare allows 120 days, and Medicaid varies by state. Two clocks run at once: the time it takes you to detect the variance and the time you have left to appeal it. A quarterly audit that finds a shortfall on day 100 leaves almost no room to file. The slower your detection, the more recoverable money expires.
Recovery rarely ends on the first letter. Build an escalation ladder for when the payer's first answer is no. Request reprocessing with the documentation attached, escalate persistent patterns to your payer relations or contracting contact as a potential contract breach, and use your state's prompt-pay statute, which requires payers to process clean claims within a set window and pay interest on late or incorrect payments. When a payer recoups already-paid claims through a third-party vendor, the burden compounds. As one practice owner, Michael Reinhorn, MD, put it:
"It's quite painful to be in a situation where a patient comes to the office with a painful lump, has surgery to fix their problem, does well, and the surgeon's practice has to spend countless hours fighting to get paid fairly."
- Michael Reinhorn, MD, practice owner
Recovering today's underpayments returns earned revenue. The data you generate doing it solves a bigger problem.
How to prevent healthcare underpayments from recurring
Preventing recurrence means feeding your underpayment data back into payer monitoring and your next contract negotiation. Every underpayment you detect is evidence, and evidence changes your position with a payer from a request to a documented claim.
Track three metrics per payer in a scorecard: the underpayment rate, the percentage of disputes resolved in your favor, and the average days to resolution. After two or three quarters, the scorecard shows which payers underpay most and gives you specifics to bring to the table. Walking into a renewal with "Payer X underpaid 8% of our claims last year, totaling a documented shortfall" turns a vague ask for higher rates into a concrete demand to pay the rates already agreed to. The deeper version of this work belongs in your payer contract negotiation strategy, where underpayment data becomes negotiating leverage.
Operational prevention closes the rest of the gap. Load new fee schedules into your system the day a contract takes effect so drift never starts. Run monitoring rules that compare every payment against expected reimbursement instead of sampling after the quarter ends. For the underlying detection process itself, including how to run a payer audit without enterprise software, see our guide to underpayment detection. The goal is to apply the same scrutiny to paid claims that your team already applies to denied ones.
Start with one payer and one expected-rate comparison
Healthcare underpayments are the quietest line item in your revenue cycle. They do not announce themselves, they do not reach a worklist, and they close as zero-balance accounts that look finished. The revenue is already yours. The only question is whether you are checking that you received it.
The first step takes an afternoon. Pick your highest-volume commercial payer, pull a sample of recently paid claims, and compare each payment against your contracted rate for that code. If the payments match, move to the next payer. If you find a pattern, you have found revenue to recover and the first data point for your next negotiation.
Share this article
Help spread the knowledge by sharing with others
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Related Articles
Continue exploring healthcare transparency and compliance topics
Multi-Specialty Coding Guide: Billing in Multi-Specialty Practices
A multi-specialty coding and billing guide for physician groups. Covers CPT, modifier 25, NPP rules, and fee schedules in multi-specialty practices.
Behavioral Health Payer Contracting: A Practice Owner's Guide
A practice owner's guide to behavioral health payer contracting: decode the contract before you sign, find out if your rate is below market, and negotiate up.
Transparency in coverage data: how providers turn the payers' own files into negotiating leverage
The Transparency in Coverage rule was marketed as a consumer shopping tool, but the files it produced let provider contracting teams see what payers pay their competitors. This guide explains what's actually in the data, why the raw files mislead you, and how to use them to benchmark your rates and strengthen your next negotiation.