Transparency in coverage data: how providers turn the payers' own files into negotiating leverage


Cameron Fletcher
Head of Growth at PayerPrice
You sit across the table from the payer at renewal, and they know something you do not. They know what they pay the hospital across town for the same DRG. They know what the physician group three miles away accepts for a 99214. You know only your own fee schedule. That asymmetry has shaped every payer contract negotiation for decades, and it has almost always worked against the provider.
The cost of that gap is real money. Daniel J. Marino, who has spent more than two decades in managed care contracting, describes the position most provider organizations find themselves in.
"They're really at a disadvantage. They feel like it's very difficult for them to build a level playing field, to have a conversation with the payers in such a way that it creates a win-win."
- Daniel J. Marino, host of Lumina's Value-Based Care Insights podcast
Since July 2022, that asymmetry has a crack in it. Federal regulation now forces payers to publish what they pay every in-network provider, in public files anyone can download. The catch is that the data was built for consumers, the files are enormous, and they are full of errors that will mislead anyone who opens them cold. This article explains what transparency in coverage data actually contains, why the raw files lie to you and how to read them anyway, how to benchmark your reimbursement against competitors, and how to bring that benchmark to the negotiating table.
What's actually in transparency in coverage data (and what isn't)
Transparency in coverage data is the set of machine-readable files that health plans must publish under the 2020 Transparency in Coverage rule, disclosing the negotiated in-network rate they pay every provider for every covered service. The rule produces two file types: in-network negotiated rates, and historical out-of-network allowed amounts. The in-network file is the one that matters for contract benchmarking, because it contains the actual dollar amount a payer has agreed to pay a named provider for a specific billing code.
The files are JSON, not PDF or spreadsheets. According to BCBS North Dakota, payers post them publicly with no account or password, update them monthly, and stamp each file with its date. They contain no patient information. They contain rates, provider identifiers, billing codes, and the network each rate applies to.
Two gaps in the data matter before you start. The prescription drug file required by the rule has been delayed indefinitely, so drug pricing is not part of what you can pull today. And payers exclude thin data: according to Johns Hopkins Employer Health Programs, pricing data with fewer than 20 rows per provider per billing modifier are dropped from the files. Sparse services for a given provider may simply not appear.
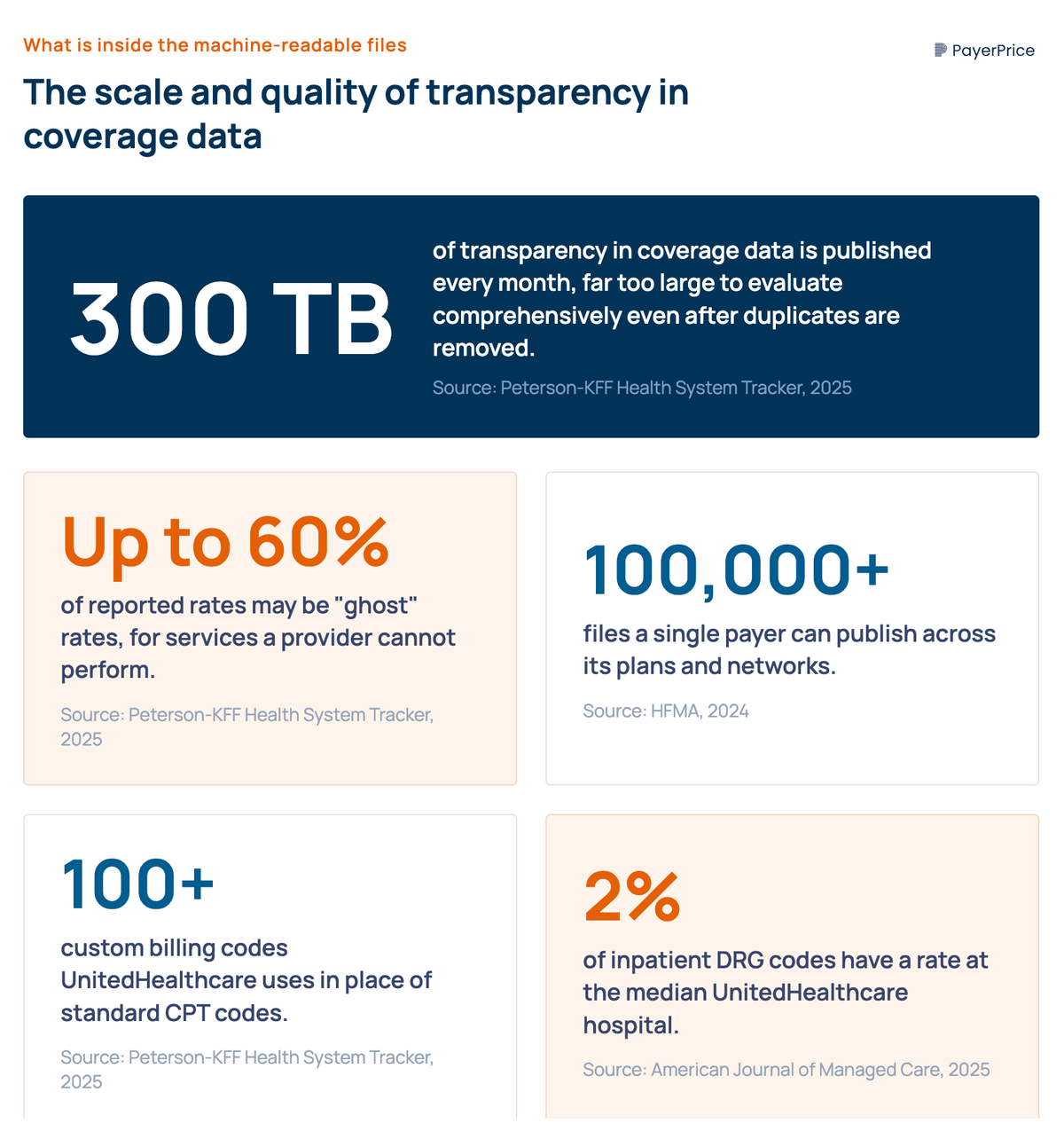
The single most important fact about this data is its size. According to the Peterson-KFF Health System Tracker, Turquoise Health, one of the organizations that aggregates these files, takes in up to 300 TB of transparency in coverage data each month, and even after duplication is removed the remaining volume is far too large to evaluate comprehensively. This is not a download-and-open situation. A single payer can publish more than 100,000 files. That scale is the first reason practitioners describe the data the way they do, and it sets up the harder problem: even once you get the files open, most of what is inside them is not what it appears to be.
Why raw transparency in coverage data will lie to you, and how to read it anyway
The raw files contain large volumes of rates that are wrong, duplicated, or impossible to compare, and a provider who treats every number as a real price will reach false conclusions. Doral Jacobsen, a managed care contracting expert, puts the practitioner experience plainly.
"There is some transparency data that's out there, but it's really hit or miss."
- Doral Jacobsen, MBA, FACMPE, on the MGMA Women in Healthcare podcast
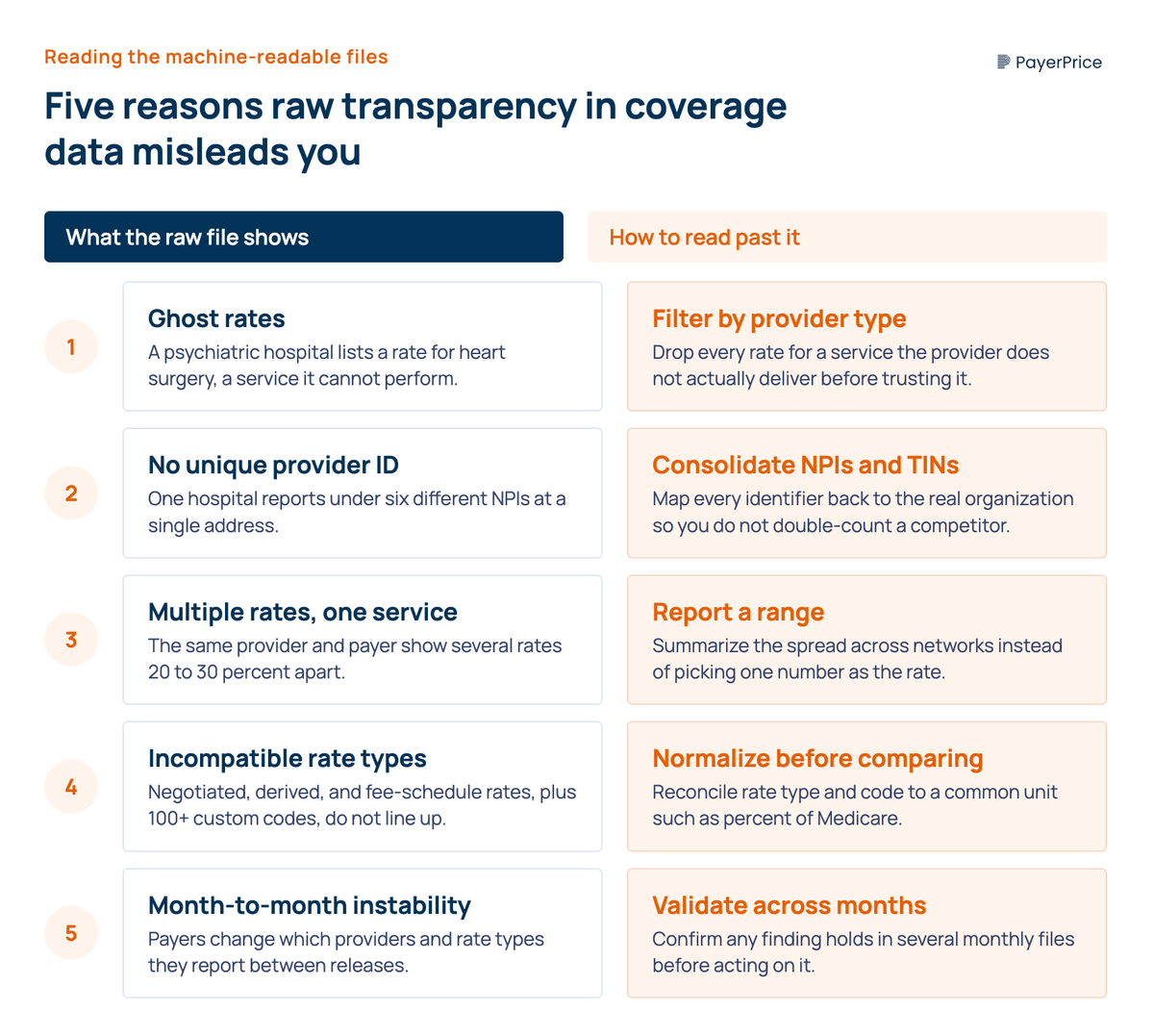
Five specific problems cause the "hit or miss" experience. Each has a defense.
- Ghost rates. Payers publish rates for services a provider cannot perform. The Peterson-KFF brief found psychiatric hospitals reporting rates for heart surgeries and urologists reporting rates for knee replacements. According to that analysis, Turquoise Health has estimated that as much as 60% of reported rates may be ghost rates. Filter every rate against what the provider type actually does before you trust it.
- No unique provider identifier. One hospital reports under many National Provider Identifiers. The Peterson-KFF analysis found UnitedHealthcare reporting rates for six different general acute care NPIs at a single New York-Presbyterian address. Average those six without consolidating and you have inflated or double-counted a single competitor. Map every NPI and TIN back to the real organization first.
- Multiple rates for the same service. The same provider, payer, and service often carries several different rates across networks, with the highest value 20% to 30% above the lowest for no stated reason. Report a range, not a single number, when you summarize a competitor's rate.
- Incompatible rate structures. Payers label rates as negotiated, derived, or fee-schedule, and report them as per-diem, case rate, percent of charges, or bundle. According to Peterson-KFF, UnitedHealthcare also replaces standard CPT codes with more than 100 custom billing codes. A per-diem rate is not comparable to a percent-of-charges rate, and a custom code does not line up against a competitor's CPT. Normalize the rate type before you compare.
- Month-to-month instability. Reporting changes between releases. Peterson-KFF documented Aetna substantially changing the number and types of providers it reported for sample CPT codes between March and July 2024. Validate any finding across several months before you act on it.
There is a sixth issue that is not a flaw to clean out but a signal to read. The data is incomplete, and the pattern of incompleteness differs by payer. According to a 2025 completeness study published in The American Journal of Managed Care, the median UnitedHealthcare inpatient hospital had negotiated rates for only 2% of DRG codes, while physician and hospital outpatient data were far more complete and usable. The same study found that UnitedHealthcare listed significantly fewer providers in its files than its marketing claims, and that Blue Cross Blue Shield plans report so inconsistently that they cannot be combined for collective analysis. Pull physician and outpatient rates for benchmarking today. Treat inpatient files as usable only if you can validate them across multiple months.
Knowing which numbers to trust is the hard part. Once you can isolate the real, comparable rates, you can answer the question that brought you to this data in the first place: how do your rates compare to your competitors'.
How to benchmark your reimbursement against competitors with transparency in coverage data
Benchmarking with transparency in coverage data means pulling each competitor's negotiated rate for the same billing code from the same payer in your market, normalizing those rates, and measuring your own contracted rate against them. Most provider organizations do not start here. They start with percent of Medicare, because Medicare rates are public and consistent. Rita Reyes-Williamson, Senior Director of Managed Care at Surgery Partners, describes the standard method.
"Medicare rates are public. You should be able to reprice in a model, and this can be Excel based. They can reprice every case that they did for Aetna against what would Medicare have paid, so you benchmark all your Aetna commercial cases, and it looks like you're performing at say 130 percent of Medicare."
- Rita Reyes-Williamson, Senior Director of Managed Care at Surgery Partners, on the HST Pathways podcast
Percent of Medicare tells you how your contract performs against a fixed federal yardstick. It does not tell you how you perform against the group down the street. Transparency in coverage data closes that gap, because it contains the competitor rate Medicare benchmarking can never show you. Here is the sequence to get from raw files to a usable comparison.
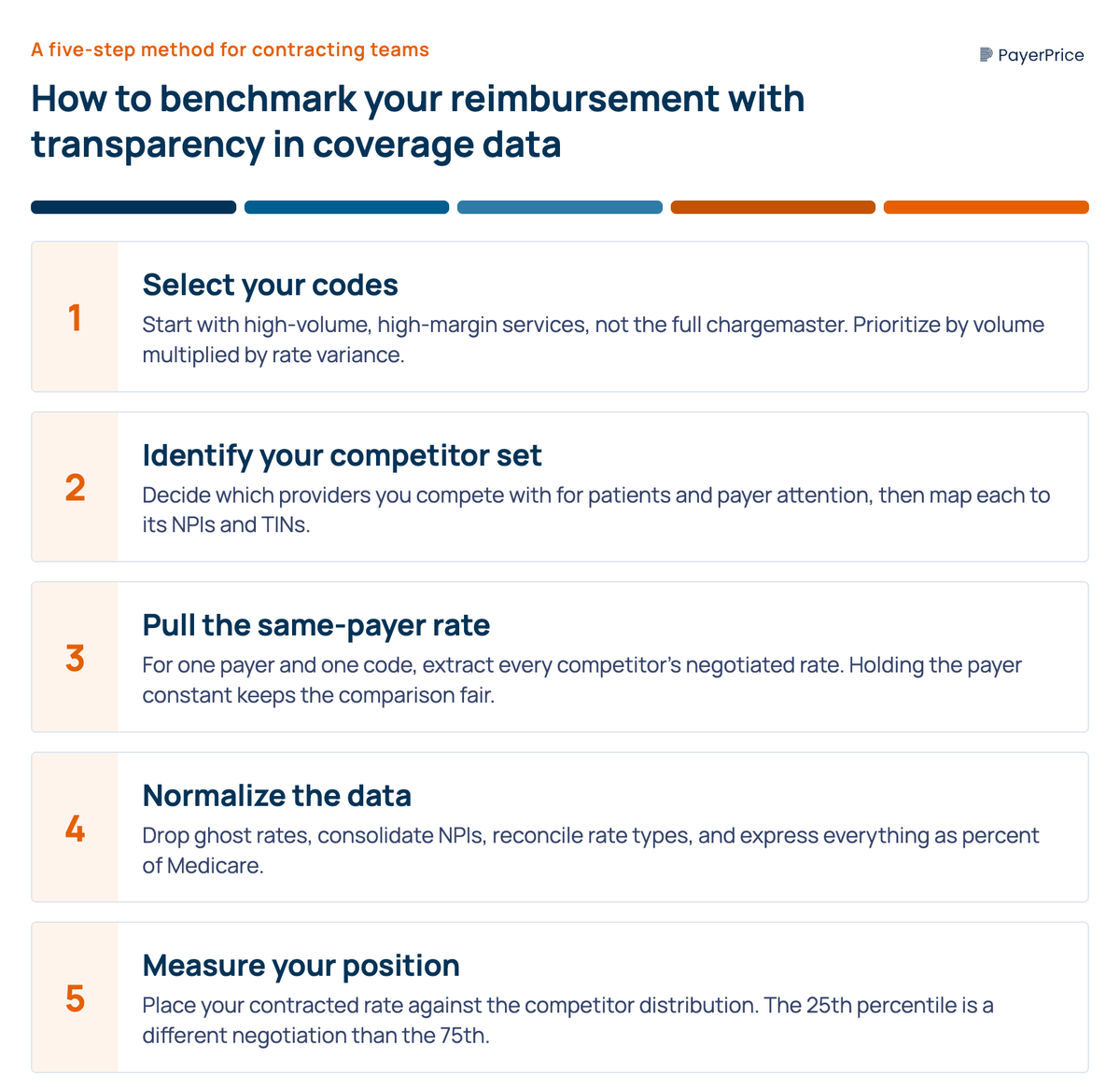
- Select your codes. Start with high-volume, high-margin services, not your entire chargemaster. Jerry DiMaso, CEO of the analytics firm Payerset, describes how providers use the data to find where it matters: for a focused set of codes, a provider learns they are under-reimbursed relative to competitors, which is where the data becomes useful. Prioritize by volume multiplied by rate variance.
- Identify your real competitor set. Decide which providers you actually compete with for patients and payer attention in your metro, then map each to its NPIs and TINs so you can find them in the files.
- Pull the same-payer rate for each competitor. For one payer and one code, extract every competitor's negotiated rate. Keeping the payer constant is what makes the comparison fair, since the same payer pays different providers differently.
- Normalize. Apply the five defenses from the previous section. Drop ghost rates, consolidate NPIs, reconcile rate types, and express everything in a common unit such as percent of Medicare.
- Measure your position. Place your contracted rate against the normalized competitor distribution. A rate at the 25th percentile of your market is a different negotiation than a rate at the 75th.
This is the analysis that turns a vague sense of being underpaid into a specific, defensible number. The next question is what to do with it.
Bringing the data to the negotiating table
A normalized competitor benchmark changes a rate negotiation from an opinion into an argument, because you can show the payer exactly where it pays competitors more for the same service. Brad Gingerich, VP of Payer Strategy at Ensemble Health Partners, describes the shift this creates.
"Price transparency allows us to actually have these conversations and speak with payers about competing providers' rates. It allows us to achieve more rate parity across the industry when you see competitors' rates and then leverage that in your negotiation."
- Brad Gingerich, VP of Payer Strategy at Ensemble Health Partners, on an HFMA contract negotiation roundtable
The rate-parity argument is direct. You bring a payer evidence that it pays a comparable competitor 20% more for the services you both deliver, and you ask for parity. Because your figure is normalized and validated across multiple months, the payer cannot dismiss it as a misread of messy data. That preparation is what separates a benchmark the payer takes seriously from one it waves away.
Rate is not your only lever, and combining it with operational evidence strengthens the position. Stephen Forney, a provider-side finance leader on the same HFMA roundtable, found that payer performance itself became a source of leverage in his last three negotiations, driven by whether the payer processes claims cleanly and acts as a good partner. Pair your rate benchmark with a payer scorecard that quantifies denials, payment delays, and claims friction. Gingerich frames the underlying principle the same way in a Becker's Hospital Review interview: data is the provider's greatest leverage.
Getting to that prepared position requires turning hundreds of terabytes of flawed JSON into a clean, defensible figure. That work is the real obstacle, and it forces a decision about how to do it.
Build versus buy: getting to usable data without a data science team
Building a transparency in coverage data capability in-house means ingesting terabytes of files every month, resolving provider identities, normalizing rate types, filtering ghost rates, and re-running the whole pipeline as payers change their reporting. That is a genuine data engineering effort, and most managed care and revenue cycle teams are not staffed for it. Damon Morse, a payer-rate analyst, describes where providers get stuck.
"A lot of groups that I work with just don't even know where to start. How do we compare to the market as it relates to our current rates and our current contracted fee schedules?"
- Damon Morse, on Lumina's Value-Based Care Insights podcast
The buy option is a platform that has already solved the ingestion and cleaning problem. When you evaluate one, hold it against the specific failure modes in the raw data. A platform worth paying for does five things.
- It normalizes rate types, so negotiated, derived, and per-diem rates are reconciled into something comparable.
- It matches providers across multiple NPIs and TINs back to real organizations, so you are not double-counting a competitor.
- It filters ghost rates rather than passing them through to your analysis.
- It handles completeness honestly, telling you when inpatient data is too sparse to trust instead of presenting 2% coverage as a market rate.
- It refreshes monthly and lets you drill to the code level for your specific competitor set.
A tool that does those five things turns a months-long engineering project into a query you run before a renewal. A tool that skips them hands you the same flawed files in a nicer interface. The distinction is whether the vendor has actually done the cleaning, or simply re-displayed the raw data.
Turning the rule against the asymmetry it was meant to fix
The Transparency in Coverage rule was sold as a way to help patients shop for care. Patients cannot use 300 TB of monthly JSON, and the data is too flawed to read without preparation. The provider contracting team that learns to read it is the one that benefits, because the files reveal the one thing the negotiating table has always hidden: what the payer pays your competitors.
Your first step does not require a vendor or a data team. Pick the three services where you do the most volume, identify the two or three competitors you care about most, and find out whether their negotiated rates with your largest payer sit above or below yours. That single comparison, done carefully and validated across a couple of months, tells you whether you are walking into your next renewal underpaid. The data exists, it is public, and for the first time the asymmetry runs in both directions.
Share this article
Help spread the knowledge by sharing with others
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Related Articles
Continue exploring healthcare transparency and compliance topics
Multi-Specialty Coding Guide: Billing in Multi-Specialty Practices
A multi-specialty coding and billing guide for physician groups. Covers CPT, modifier 25, NPP rules, and fee schedules in multi-specialty practices.
Healthcare Underpayments: A Provider's Recovery Guide
Healthcare underpayments hide as zero-balance claims no worklist ever flags. See how providers detect, recover, and prevent the revenue payers quietly keep.
Behavioral Health Payer Contracting: A Practice Owner's Guide
A practice owner's guide to behavioral health payer contracting: decode the contract before you sign, find out if your rate is below market, and negotiate up.