Multi-Specialty Coding Guide: Billing in Multi-Specialty Practices
A multi-specialty coding and billing guide for physician groups. Covers CPT, modifier 25, NPP rules, and fee schedules in multi-specialty practices.


Cameron Fletcher
Head of Growth at PayerPrice
Multi-Specialty Coding Guide: Billing in Multi-Specialty Practices
Your new client is a 14-physician multi-specialty practice. Internal medicine, cardiology, orthopedics, and behavioral health under one TIN. Net collection rate 91 percent, same-day claim denials climbing, and two physicians who joined six months ago whose charge volume started two months late. You have 90 days to identify whether the leak is in coding, contracting, or credentialing.
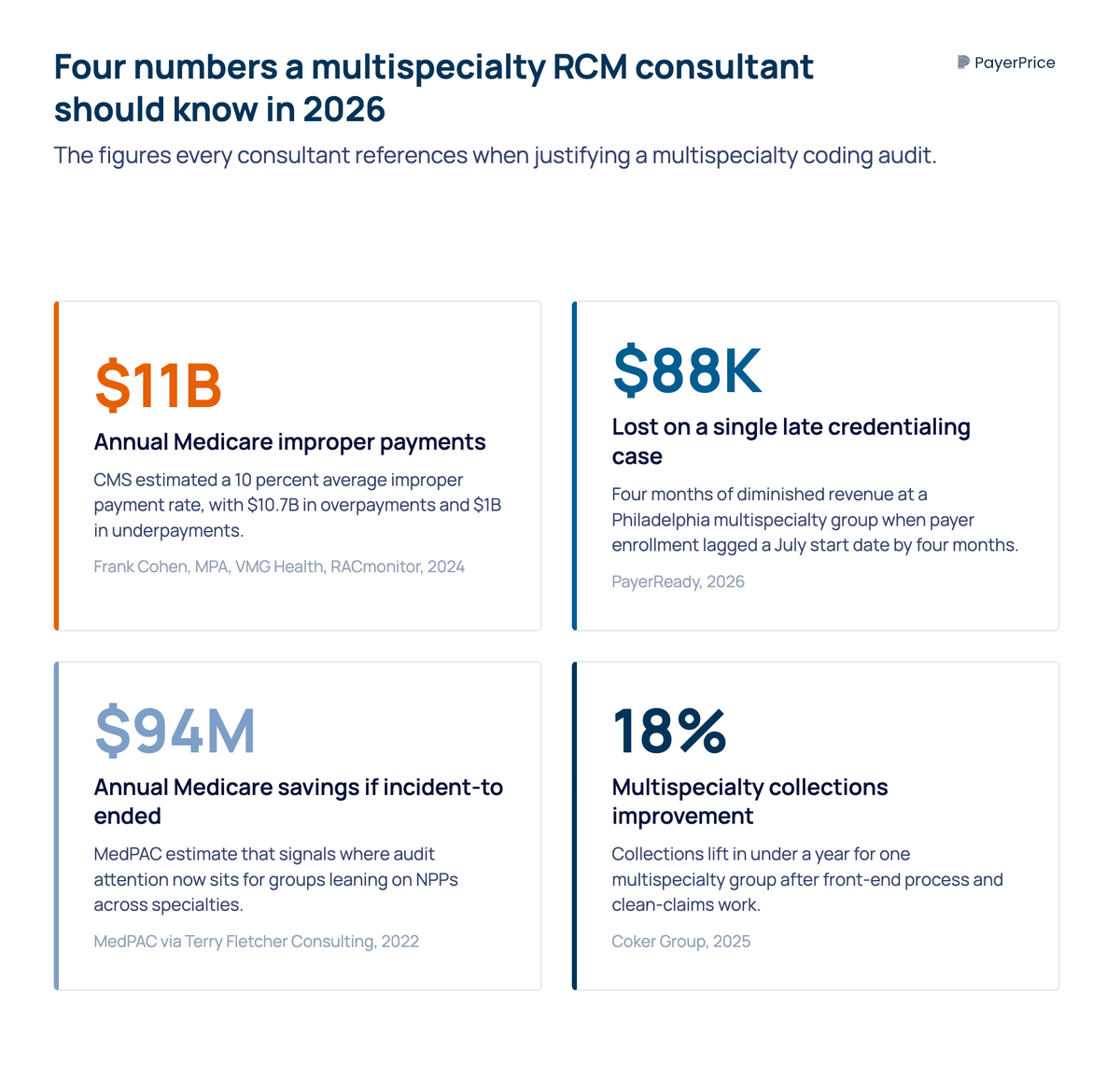
According to RACmonitor, CMS estimated a 10 percent improper payment rate on the period Frank Cohen, MPA, Senior Director of Analytics at VMG Health, analyzed, totaling roughly $11 billion. In a multi-specialty group, the gap multiplies. Each practice line carries a different CPT mix, modifier conventions, NPP rules per MAC, and credentialing requirements per payer. The complexities of multi-specialty billing compound at every layer.
This comprehensive guide is the diagnostic order an experienced RCM consultant follows on intake. Seven chapters: coding guidelines, billing for services across multiple specialties, NPP rules, fee schedule loading, and the first-90-days checklist that helps healthcare providers improve reimbursement.
The Medicare rule that governs every multi-specialty coding decision
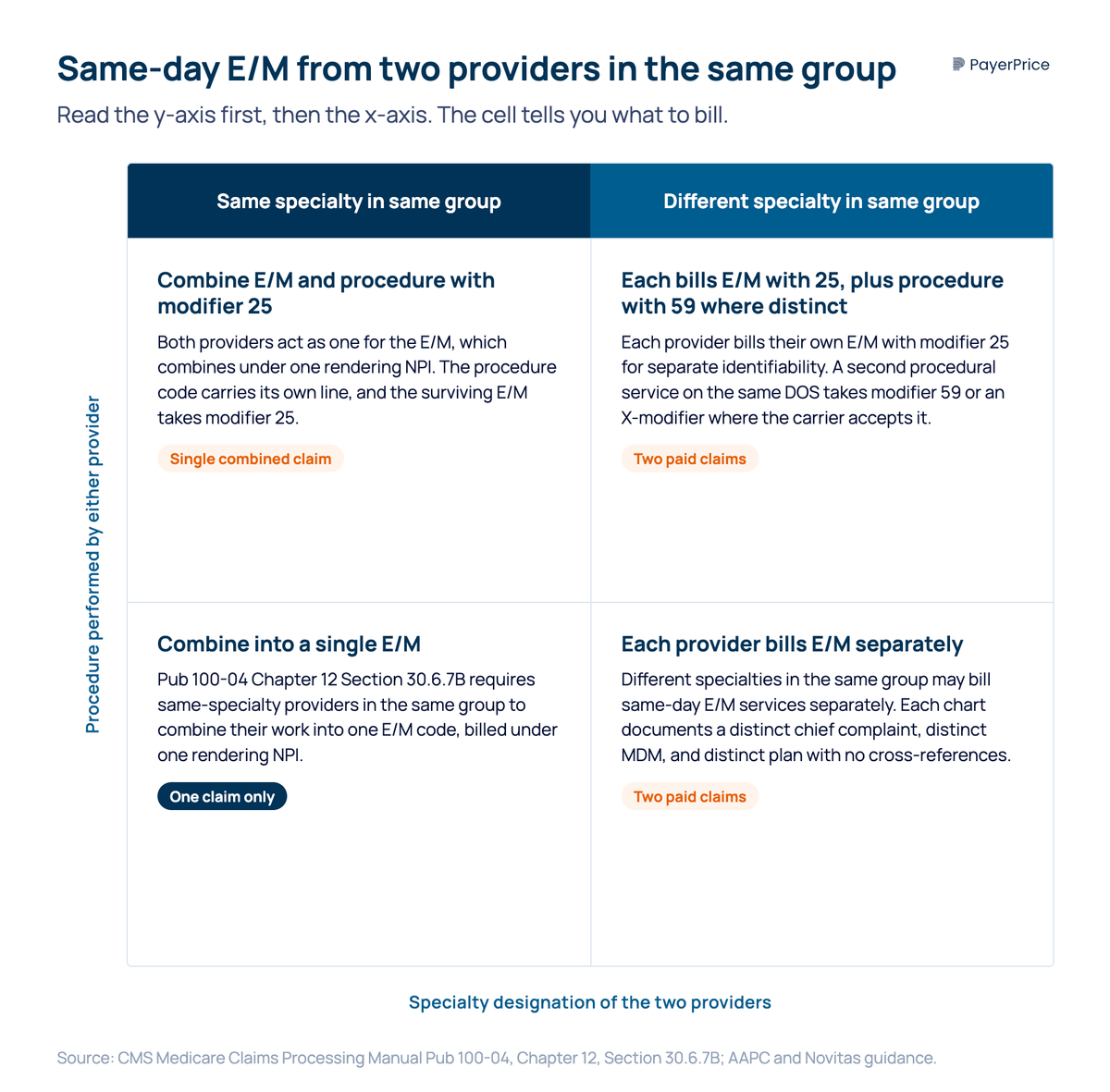
The single rule is Medicare Claims Processing Manual Pub 100-04 Chapter 12 Section 30.6.7B: physicians of different specialties in the same group practice may bill same-day evaluation and management services separately, while physicians of the same specialty in the same group must combine into one evaluation and management code. Every modifier convention, NPP question, and same-day denial appeal flows from how that rule meets carrier edit logic.
The administrative definition is Medicare Specialty Code 70, which crosswalks to NPI taxonomy 193200000X. Confirm the practice is enrolled at the entity level and each physician under their individual line taxonomy. A missing taxonomy at the physician level silently routes claims to the wrong fee schedule.
The IRS group definition is the TIN, not the practice name. Two entities under separate TINs in the same single location are two physician groups for billing purposes.
New patient visits and established patient visits in the same group
The new and established patient three-year rule applies at the specialty and sub-specialty level, not the group level. According to the California Medical Association, a patient seen by a general surgeon in 2014 and an internist in the same group in 2016 codes as a new patient encounter for the internist because the practice lines differ. Current Procedural Terminology guidelines from the American Medical Association treat the specialty of the physician as the trigger, not the practice name.
Three rules every consultant memorizes for new or established determinations:
- A patient who received a service from a physician of the same specialty within the group in the past three years is an established patient. Two physicians of the exact same specialty are treated as one for new patient codes.
- A patient seen by a different practice line in the group, with no face-to-face from that line in three years, qualifies for the new patient visit codes.
- NPs and PAs assume the supervising physician's specialty for new patient determinations, with one MAC-level exception in chapter 5.
The medical record is the only thing that survives an audit.
Same-day E/M billing for two specialists in the same multi-specialty practice
The most common denial pattern is two specialists in the same group billing patient E/M services on the same day, with the carrier denying as duplicative even though Pub 100-04 §30.6.7B authorizes both. The fix is operational.
A working biller posted the field reality on Codapedia:
"Example 1: Two orthopedic visits (same day with two diags). Example 2: One primary care visit, one ortho visit, one cardiology visit. These are not getting paid. We have tried submitting with modifiers 25 and 27 but still get denied."
- Stacey, group practice biller, Codapedia practitioner forum
Most carrier edits compare rendering provider, service date, and TIN, treating the second claim as a duplicate. According to a 2023 AAPC Discuss thread citing the Novitas FAQ, physicians in the same group but in different specialties may bill and be paid separately.
The operational fix has four moving parts.
- Distinct diagnosis code sequencing per practice line. Each E/M lists a presenting problem inside that scope. Where two specialists share an underlying condition, each documents a distinct chief complaint, distinct medical decision making, and distinct plan.
- Modifier 25 on each E/M paired with a procedure. Where a clinician performs a minor procedure on the same day, the patient E/M carries a 25 modifier to flag it as significant and separately identifiable from services rendered.
- No cross-reference documentation. An internist who writes "defer to cardiology" gives the auditor a duplication argument. Each chart stands alone with distinct medical necessity language.
- A single-page appeal letter. Cite Pub 100-04 §30.6.7B, name the carrier's provider manual section, attach two redacted notes, and request reprocessing. Most commercial carriers reverse on the second pass.
Quarterly audits of same-day claim denials by practice-line pair, with the appeal template instantiated in the practice management system, move consultant work from one-off recovery to a recurring revenue process.
Modifier 25 audit exposure across the group
Modifier 25 is the most-audited modifier in medical coding, and the group setting multiplies the audit exposure by stacking 25 across providers, multiple specialties, and same-day procedures.
According to Terry Fletcher Consulting on the February 24, 2026 CodeCast podcast:
"Modifier 25 remains one of the most audited and most overused modifiers in medical coding. But the problem isn't just coding mechanics. It's about appropriateness, credibility, and documentation."
- Terry Fletcher, CPC, CCC, CEMC, host of CodeCast and NSCHBC consultant
Fletcher predicted the 2022 policy shift that has now landed:
"Many payers are starting to put restrictions on payment and submission requirements when billing the 25 modifier on E/M services with minor procedures on the same date. You will see reductions in payments and new paperwork requirements."
The unique billing exposure compounds in four ways:
- Procedure plus E/M, same provider. The classic 25 use case. Document the procedure separately, support the E/M with distinct MDM, append 25.
- Procedure plus E/M, two different specialists in the same group. Each claim stands on its own documentation. Carrier edits that aggregate by TIN deny anyway.
- Modifier 59 on a separate procedural service. Where two clinicians each perform a procedure on the same DOS, the second procedure may carry 59 to identify a distinct service.
- NPP-billed E/M with 25. Where the next chapter's split/shared and incident-to rules collide with the E&M codes covered here.
A consultant audit on 25-flagged encounters checks for separately identifiable services, distinct chief complaint, global period handling, modifier placement, and chart independence. The output is the percentage at audit risk, which is the basis for the policy change next.
Medicare patient NPP rules: split/shared, incident-to, and group practice billing
The 2024+ split/shared substantive-portion rule rewrote how facility-based visits between an MD and an NPP are billed inside a group practice. Three rules govern NPP billing.
Split/shared visits in the facility setting. According to E&M Consulting summarizing the 2026 final rule:
"Split-shared visits are only allowed in the facility setting. If based on time, combine the time between the APP and the physician to determine the code. The visit should then be billed under whoever spent more than half of the total time. When billing split shared services, an FS modifier should be added."
- E&M Consulting, summary of the 2026 final rule
Incident-to in the office setting. Incident-to allows an NPP encounter to bill under the supervising physician's NPI at 100 percent of the physician fee schedule, where the NPP follows an established plan of care, the supervisor is in the suite, and the patient encounter is for an established problem. Terry Fletcher Consulting noted MedPAC has estimated annual savings of more than $94 million in reimbursement if incident-to were eliminated. Compliance exposure sits on supervision documentation, scope of practice, and the established-problem requirement.
The Noridian subspecialty-declaration rule. According to Noridian Medicare Jurisdiction F, effective March 1, 2022, NPPs must include subspecialty information in the 2400 NTE loop or Box 19 of the CMS-1500 to avoid same-day and three-year same-line edits. A cardiology NP whose claim does not declare cardiology is processed as if the NP shares the exact same specialty as every other NP in the group.
This contradicts AAPC and CMA medical association guidance that NPPs assume the supervising physician's specialty. Both rules are correct in context. The intake answers five questions: which MAC, what setting mix, how time is captured, who signs the substantive portion, and whether subspecialty is declared.
Fee schedule loading and the underpayment diagnostic
Practice management systems frequently load one fee schedule for the whole TIN and silently underpay practice lines whose rates are pegged to a different conversion factor or carve-out. The diagnostic is a CPT code-by-line paid-versus-contracted variance pivot.
A 14-physician group with internal medicine, cardiology, orthopedics, and behavioral health may be paid internal medicine E/M at the contracted base rate and cardiology procedures at 130 percent of that base. If the medical billing software carries one rate table per CPT code, cardiology procedures post at the internal medicine rate and the 130 percent carve-out evaporates silently every month.
According to Becker's Hospital Review, Carrie Laureano-Meggett, Project Manager Physician Billing at Coronis Health:
"Multi-specialty groups need more than dashboards. They need reporting that helps leaders understand what is changing, where risk is building and which actions will improve performance."
- Carrie Laureano-Meggett, Project Manager Physician Billing, Coronis Health
No results
Adjust your filters or try a different code.
The week-one diagnostic has three layers:
- Pull a 90-day claims extract by CPT code, line of practice, carrier, contracted rate, and paid amount.
- Build a paid-versus-contracted variance pivot. The top 20 dollar-variance lines are where loaded-schedule errors live.
- Cross-reference variance lines against the contract document. Where the contract specifies a carve-out the loaded schedule misses, the claim is recoverable through an underpayment letter.
The credentialing layer feeds this leak. According to PayerReady, one Philadelphia practice lost approximately $88,000 in four months when payer enrollment lagged a July 1 start date. The credentialing-to-billing handoff diagnostic answers four questions per physician: is taxonomy 193200000X registered with every contracted insurer; is each individual line taxonomy registered; is CAQH current per specialty and sub-specialty; are effective dates aligned to the start date. A missing individual taxonomy routes the claim to the wrong fee schedule even after the group taxonomy clears.
Where this leak ends, contract enforcement begins. Closing coding leaks in 90 days builds the case for contract work next, and the healthcare contract negotiation playbook picks up where this audit ends.
First-90-days checklist and when medical billing services help
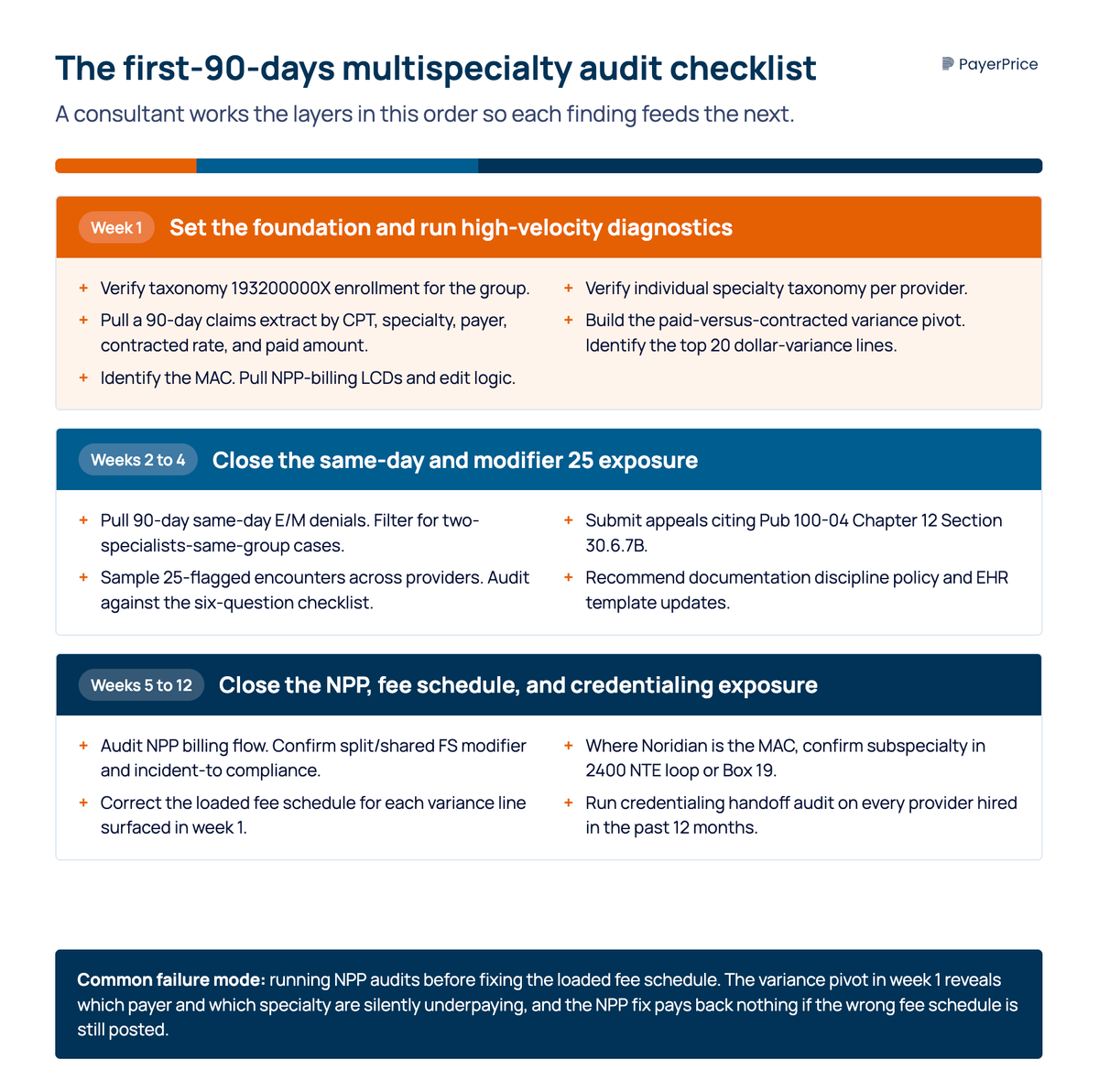
Each layer feeds the next. The first-90-days checklist runs in three week-banded phases.
Week 1. Verify enrollment under taxonomy 193200000X and individual line taxonomies. Pull a 90-day claims extract by CPT, line, carrier, contracted rate, and paid amount. Build the variance pivot. Identify the MAC and pull NPP-billing LCDs and the codes and payer rules that govern them.
Weeks 2 to 4. Pull same-day E/M claim denials. Filter for two-specialists-same-group cases. Submit appeals citing Pub 100-04 §30.6.7B. Sample 25-flagged encounters and audit against the coding compliance checklist. Recommend documentation policy and EHR template updates that close coding errors at the source.
Weeks 5 to 12. Audit NPP billing against the five-question intake. Confirm split/shared FS modifier in the facility setting and incident-to compliance in the office setting. Where Noridian is the MAC, confirm subspecialty in 2400 NTE loop or Box 19. Correct the loaded fee schedule for each variance line. Run the credentialing handoff audit on every physician hired in the past 12 months.
When do outsourced medical billing services help? The complexities of billing across the group rarely fit a single in-house team beyond four lines. Medical billing in multi-specialty practices outsourced under line-aligned billers scales coding requirements the practice cannot hire. Billing for multi-specialty clinics with shared coders works at two or three lines; beyond that, line-aligned outsourcing wins. Either model only works once the loaded fee schedule is correct and coding requirements are documented.
Coding requirements at the front end and contract enforcement at the back end are the same revenue problem from two ends.
Share this article
Help spread the knowledge by sharing with others
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Related Articles
Continue exploring healthcare transparency and compliance topics
Transparency in coverage data: how providers turn the payers' own files into negotiating leverage
The Transparency in Coverage rule was marketed as a consumer shopping tool, but the files it produced let provider contracting teams see what payers pay their competitors. This guide explains what's actually in the data, why the raw files mislead you, and how to use them to benchmark your rates and strengthen your next negotiation.
Independent Clinical Laboratory Coding: CPT® Codes & Billing
Independent clinical laboratories CPT coding & billing: Current Procedural Terminology codes, payer reimbursement, administrative service codes, medical services.
Ophthalmology & Retina Coding Guide: Billing & Coding
2026 ophthalmology and retina coding guide for the retina practice. CPT codes, billing and coding, diagnostic imaging, cataract, ophthalmic reimbursement.