Healthcare Payer Contract Negotiations: The Physician Group Playbook for Better Reimbursement
37% of physician groups never negotiate payer contracts. Learn the benchmarking methods, contract clauses, and tactics that close the reimbursement rate gap.


Cameron Fletcher
Head of Growth at PayerPrice
Healthcare Payer Contract Negotiations: The Physician Group Playbook for Better Reimbursement
A 40-physician multi-specialty group discovers during a routine consultant review that its top insurer reimburses 15% below the regional average for the same CPT codes. The contract has auto-renewed three times. Nobody on staff questioned the rates because nobody had the data to compare them.
This is not an outlier. According to the Physicians Practice 2024 Payer Scorecard, 37% of medical practices never negotiate their payer contracts at all. Among those that do, most focus on rate bumps without examining the contract language that quietly erodes the value of those rates through downcoding, recoupment clawbacks, and unilateral policy changes.
The result is a compounding revenue leak. According to MGMA, even a 2-3% increase from a single heavily-represented payer translates to $500,000 or more in annual revenue for a mid-size practice. Multiply that across 20-30 payer contracts, and the gap between what physician groups earn and what they deserve grows into millions.
This guide covers the four things healthcare providers need to close that gap: market rate data, contract language literacy, a negotiation timeline, and the leverage analysis to secure favorable reimbursement rates.
Why most physician groups negotiate payer contracts from a disadvantage
Physician groups enter payer contract negotiations at an information disadvantage because insurance companies hold detailed rate data across their entire provider network, while individual groups rarely know how their reimbursement rates compare to the market.
Mark Schroeder, VP of Growth at Aroris Healthcare and a former UnitedHealthcare executive with 8 years on the payer side, explains the scale of this blind spot:
"You could be 15 percent behind market if you don't know where market sits from a data standpoint."
- Mark Schroeder, Aroris Healthcare (DocBuddy Journal podcast)
The problem compounds over time. Daniel Marino, Managing Partner at Lumina Health Partners with over 20 years of contract negotiation experience, describes fee schedules still active today that are "a derivative of something from 2018, or 2020" - rates that were already outdated before the post-pandemic cost surge hit physician practices.
Damon Morse, Principal at Lumina Health Partners, sees the same pattern across his client base:
"A lot of these small to mid-size organizations, they're not sure where to even start."
- Damon Morse, Lumina Health Partners podcast
The data gap is one problem. Bandwidth is another. According to Physicians Practice, the average medical practice manages 20 to 30 contracts with payers at any given time, typically with a single administrator handling all of them alongside billing, credentialing, HR, and daily operations. Hospitals employ entire managed care departments for negotiating contracts. Physician groups assign it as a side responsibility, which threatens both financial stability and their bargaining power at the table.
Payers benefit from this imbalance. Tracy Watrous, VP of Member Services at MGMA, puts it plainly: it is not in a payer's financial interest to initiate a renegotiation. Contracts sit on auto-renewal for years, and payers have no incentive to change payment rates unless the healthcare provider forces the conversation.
That information gap has a fix. The next step is building a data-driven case that makes payers respond.
How to build your negotiation case with data
The foundation of any payer contract negotiation is a rate comparison that shows exactly where your reimbursement sits relative to market. Without this, every ask is a guess, and payers treat guesses as wish lists.
Identify your top CPT codes and revenue drivers
Start with the 20 CPT codes that generate the most revenue for your medical services. For each code, pull the following per payer:
- Total claims volume over the past 12 months
- Billed amount per claim
- Actual reimbursement received per claim
- Difference between billed and collected (the contractual adjustment)
This analysis reveals which codes drive your revenue and which payers underpay relative to others. A payer mix analysis by volume and revenue helps prioritize which contracts deserve attention first.
Benchmark against market rates
Once you know your own rates, compare them against four external benchmarks:
- PayerPrice parsed the machine-readable files from different payers into searchable rate comparisons across 10,000+ health plans, so you can see precisely what a payer reimburses your competitors for the same CPT codes.
- CMS fee schedules serve as the floor. Medicare rates establish the baseline, and commercial rates are typically expressed as a percentage of Medicare (e.g., 120% of Medicare for office visits). If a commercial payer reimburses below Medicare for any code, that contract has a clear problem.
- Price transparency data from the Transparency in Coverage Act gives you something none of the above sources offer: the actual negotiated rates between specific payers and specific providers in your market.
This last data source changes the negotiation dynamic entirely. When a payer rep claims your payment rates are already competitive, you can point to specific, evidence-based analytics showing otherwise.
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Quantify your value to the payer
Rate data tells you where you stand. A value analysis strengthens your negotiating position by telling the payer why you deserve more. Compile these four elements into your negotiation proposal:
- Patient volume and panel size. How many covered lives does your group serve for this payer? If you represent 30% of a payer's primary care access in your region, that is leverage.
- Quality metrics. MIPS scores, patient satisfaction ratings (CAHPS), and clinical outcomes data (readmission rates, A1C management, cancer screening rates) demonstrate value beyond volume.
- Geographic coverage. If your group is the only multi-specialty practice within a 30-mile radius, the payer's network adequacy depends on your participation.
- Referral network. A physician group that generates referrals, imaging, lab work, and surgical volume within the payer's network saves that payer money compared to out-of-network leakage.
Payer intelligence tools help quantify these factors with actual claims data rather than estimates.
Data alone does not get contracts signed. The language inside the contract determines whether the rates you negotiate actually translate to revenue.
The contract clauses that cost physician groups the most
The clauses buried in payer contracts cost physician groups more than low rates do, because they allow payers to reduce effective reimbursement without ever renegotiating the fee schedule.
Scott Dewey, Chief Managed Care Officer at PayrHealth, describes these as "hidden trapdoors" in Medical Economics. He tells the story of a physician practice owner who negotiated what looked like a strong deal: 100% of Medicare fee-for-service rates from a major Medicare Advantage payer. Then the denials started. The payer downcoded claims based on administrative criteria that did not reflect clinical reality, and the practice's actual reimbursement fell well below the promised rate.
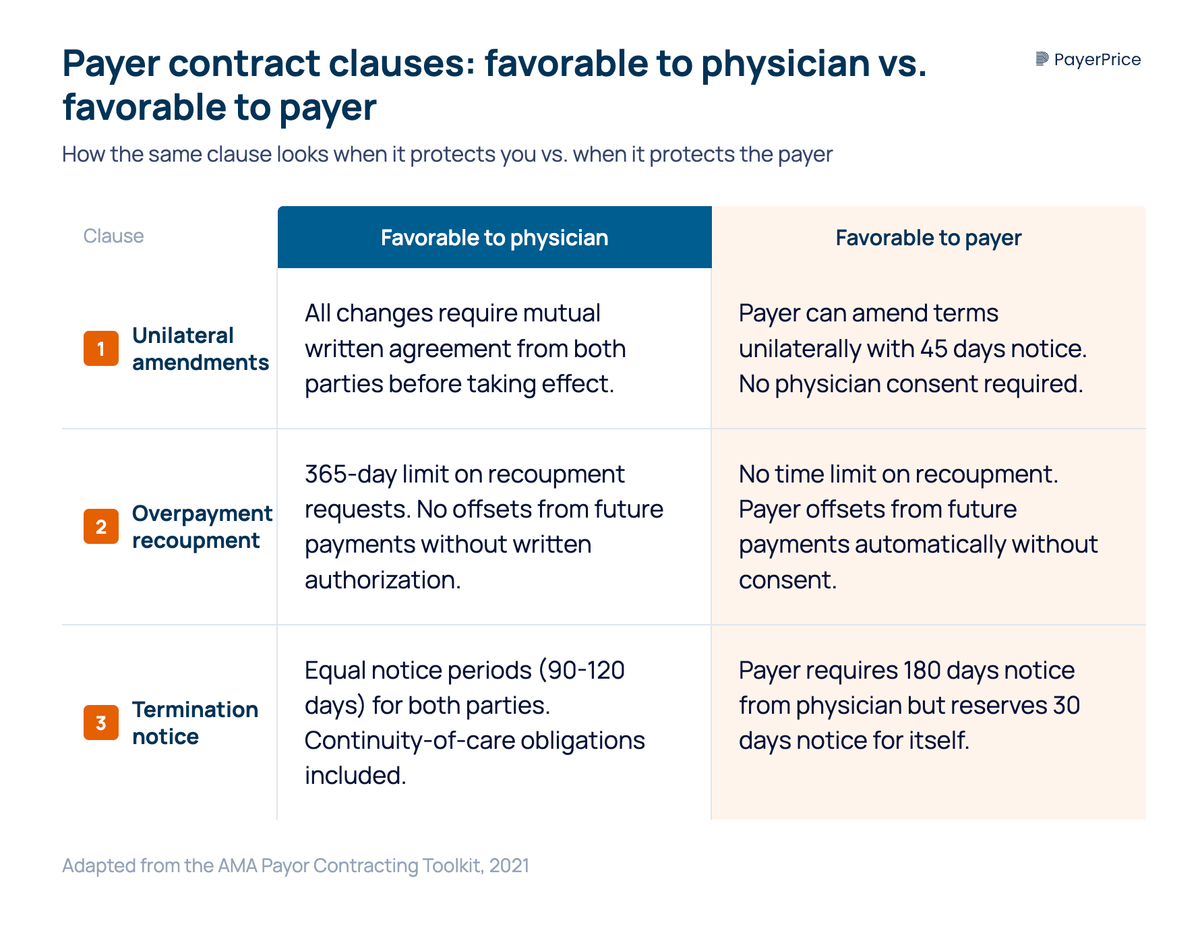
The AMA's Payor Contracting Toolkit provides side-by-side contract language comparisons showing "favorable to physician" vs. "favorable to payor" versions of the same clauses. Here are the five clauses that cost physician groups the most, drawn from that toolkit:
1. Unilateral amendment clauses. A payer-favorable version allows the payer to amend contract terms unilaterally with 45 days notice. A physician-favorable version requires mutual written agreement for any changes to ensure compliance with the original terms of reimbursement. Sheri Chatterson, VP of Payer Relations at OneOncology with 25 years in the healthcare industry, has seen this firsthand: payers are writing language that lets them expand requirements without provider consent.
2. Overpayment recoupment with no time limit. A payer-favorable version gives the payer unlimited time to request recoupment and allows offsets from future payments without consent. A physician-favorable version sets a 365-day limit on recoupment requests and prohibits offsets without written authorization.
3. Downcoding provisions. These allow payers to change coding criteria administratively, reducing payment on the same services without changing the published fee schedule. The AMA toolkit documents real examples: payers downcoding E/M visits, bundling distinct procedures into single payments, and requiring step therapy for specialty drugs.
4. Termination provisions. One-sided notice periods favor the payer. A physician-favorable contract requires equal notice periods (typically 90-120 days) for both parties and includes continuity-of-care obligations for patients in active treatment.
5. Auto-renewal (evergreen) clauses. These are the reason contracts go years without review. The contract renews at the same rates indefinitely unless one party formally objects before a specific deadline, often buried in the agreement.
Review every active payer contract for these five clauses before your next negotiation. If the language favors the payer on three or more, the contract terms are reducing your effective reimbursement regardless of the fee schedule.
Fixing contract language requires a negotiation strategy that goes beyond asking for higher rates.
Payer contract negotiation tactics that work for physician groups
Successful healthcare payer contract negotiations for physician groups require starting early, negotiating the full contract (not just rates), and knowing exactly when to walk away.
Start 12 months before expiration
According to HFMA, healthcare providers need to initiate the payer contract negotiation process a full 12 months before the contract renewal date. This is not conservative advice. Schroeder notes that the average negotiation involves "80 to 100 touch points with a payer, multiple proposals, multiple phone calls."
Payers use time as leverage. Scott Ellsworth, President of Ellsworth Consulting and author of the HFMA analysis, explains that payer contractors often lack urgency deliberately. They lead with their own objectives, push providers into reactive positions, and benefit from delays that push past auto-renewal deadlines.
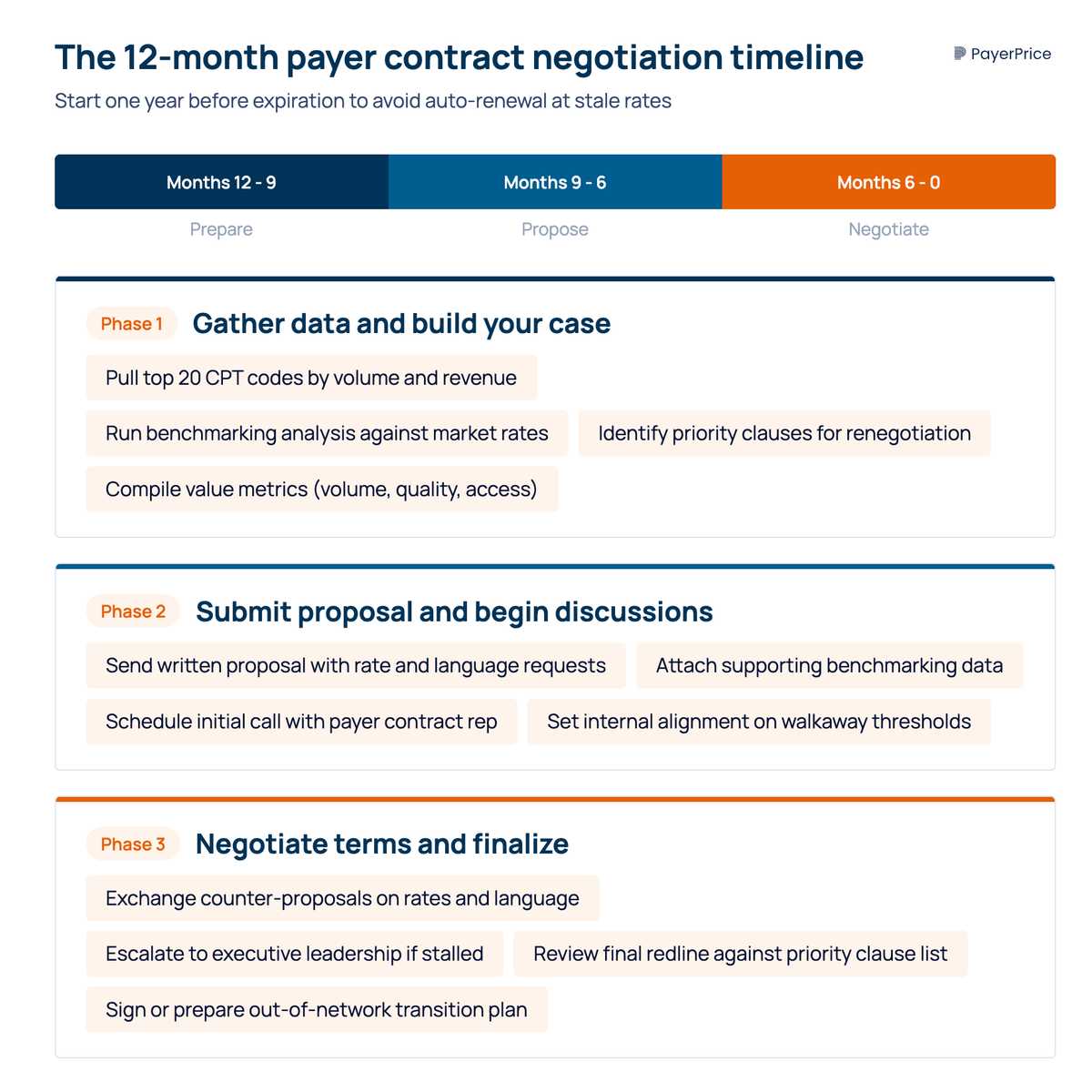
The 12-month timeline breaks down into three phases:
- Months 12-9: Gather data on your top codes, run benchmarking analysis, identify priority clauses for renegotiation
- Months 9-6: Submit initial proposal with supporting data, begin discussions
- Months 6-0: Negotiate terms, escalate to executive leadership if needed, finalize or prepare for out-of-network transition
Negotiate beyond rates
Rate increases matter, but five other contract terms directly affect how much revenue your group actually collects:
- Prompt payment terms with specific penalties for late payment (e.g., 1.5% monthly interest after 30 days)
- Prior authorization reduction or gold-carding provisions for high-performing providers. According to the Physicians Practice 2026 Payer Scorecard, 84% of practice leaders report that prior authorization requirements increased year-over-year
- Appeal rights and timelines that give your billing team a realistic window to dispute denied claims
- Medical necessity definitions aligned to clinical guidelines rather than payer-created administrative criteria
- Denial and recoupment guardrails including time limits on recoupment requests and prohibitions on automatic offsets
Each of these terms has a dollar value that directly affects your revenue cycle. A practice that negotiates a 3% rate increase but accepts unlimited recoupment rights and expanded prior auth requirements nets less revenue than a practice that holds rates flat but fixes those two provisions.
Know your walkaway point
Every negotiation requires a break-even calculation. Determine the minimum reimbursement rate per payer that covers your cost of delivering care, and know what percentage of your patient panel each payer represents.
Dr. Barbara Slager, President of Coastal Women's Healthcare in Maine, made the decision to terminate her practice's agreement with Anthem after determining that Anthem's reimbursement rates made continued participation unsustainable, with operational costs rising faster than the insurer's payment rates. Anthem held approximately 38% of the practice's patient panel and used that concentration as leverage to maintain low rates.
"They're relying on us being scared of that. It's that or go out of business."
- Dr. Barbara Slager, Coastal Women's Healthcare (News Center Maine)
Not every group can absorb a 38% panel disruption. That is exactly why the break-even analysis matters. If your practice cannot survive without a particular payer, that payer has structural leverage, and the negotiation strategy needs to account for it.
The HFMA analysis offers a critical guardrail: never use termination as a bluff. Enter the contracting process with genuine intent to reach a mutually beneficial agreement, but with full preparation for going out of network if the terms are unacceptable. Payer reps recognize empty threats, and bluffing destroys credibility when renewing contracts in the future.
Close the rate gap before your next renewal
The biggest risk for a physician group is not a failed negotiation. It is the negotiation that never happens. Every year a contract auto-renews without review, the gap between your rates and market rates grows wider.
Here is a three-step starting point you can act on this week:
- Pull your top 20 CPT codes by payer. Calculate actual reimbursement per code and identify which payers underpay relative to others.
- Benchmark those rates against market. Use MGMA data, CMS fee schedules, and price transparency data to see exactly where you stand.
- Start reviewing contracts with your five highest-revenue payers. Check for the five costly clauses outlined above: unilateral amendments, unlimited recoupment, downcoding provisions, one-sided termination, and auto-renewal deadlines.
That strategic approach gives you the foundation for a data-driven conversation with any payer. The practices that close the rate gap are the ones that show up to negotiate payer contracts with rate comparisons payers cannot dismiss, a favorable contract language request they cannot ignore, and a clear understanding of what their participation is worth.
Share this article
Help spread the knowledge by sharing with others
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Related Articles
Continue exploring healthcare transparency and compliance topics
Underpayment Detection for Physician Groups: How to Find the Revenue Your Payers Owe You
Physician groups lose 5-7% of net revenue to payer underpayments hidden in zero-balance claims. Learn how to detect patterns and recover what you're owed.
How to Use TiC Data to Negotiate Better Payer Contracts: A Guide for Physician Groups
Learn how physician groups can use Transparency in Coverage negotiated rate data to benchmark rates, build payer-ready analyses, and win contract increases.
How to Model a Payer Contract: A Provider's Guide
See how providers model payer contracts against real claims to catch a money-losing deal before signing. Formulas, a worked example, and a 5-step method.