Payer Contract Management for Medical Groups: How to Audit, Benchmark, and Renegotiate Your Contracts
Physician groups lose revenue to payer contracts silently, through underpayments and neglected renegotiations. Here's the payer contract management system to fix it.


Cameron Fletcher
Head of Growth at PayerPrice
Payer Contract Management for Medical Groups: How to Audit, Benchmark, and Renegotiate Your Contracts
Your billing system says you're collecting everything you're owed. It's wrong. When a payer remits a payment that is 5% below the contracted allowable, the claim settles as a zero-balance transaction. No alert fires. No flag gets raised. The money just disappears.
According to MGMA, physician groups lose between 7-11% of net revenue to underpaid and unpaid claims. For a $5 million practice, even a 2% underpayment rate adds up to $100,000 in lost revenue per year. And that is just the claims where the payer pays less than the contracted rate. It does not account for contracts that were poorly negotiated in the first place.
According to the Physicians Practice 2024 Payer Scorecard, 37% of practices do not negotiate their payer contracts at all. Of those that do, many accept headline rate increases without analyzing whether those increases translate to actual revenue. This article gives physician groups a four-step system for managing payer contracts: audit your existing portfolio, benchmark your rates against market data, negotiate with data instead of hope, and monitor payer performance after signing.
Why payer contract management is different for physician groups
Physician groups sit in a structural gap that hospitals and solo practices do not face. Hospitals staff dedicated managed care departments with analysts, attorneys, and contracting specialists. Solo practitioners typically accept standard rates. Physician groups, managing an average of 20 payer contracts per practice according to CAQH, handle this work with an office manager who also oversees HR, credentialing, and scheduling.
This resource gap creates a cascade of problems. Contracts go years without review. According to an MGMA Stat poll of 389 medical group leaders, 17% do not review their contracts regularly. Some contracts sit untouched for five or six years.
"A lot of groups just might not have the resources that it takes to dig into those negotiations and look at their contracts."
- Mark Schroeder, VP of Growth at Aroris Healthcare (former UnitedHealthcare executive)
The problem runs deeper than time constraints. Many practice leaders carry a psychological barrier that Doral Jacobsen, CEO of Prosper Beyond and a frequent MGMA speaker, calls the "courage gap".
"Our practices sometimes get run over by payers. We're afraid; we think that we can't ask for a raise."
- Doral Jacobsen, CEO of Prosper Beyond
According to Jacobsen's analysis in Physicians Practice (March 2026), this defeatist mindset traces to three interconnected problems: a poor track record that breeds anxiety, an absent strategy that erodes confidence, and a fundamental lack of clarity about how existing contracts are actually performing.
Clarity starts with knowing exactly where your contracts stand today.

How to audit your payer contract portfolio
A payer contract audit answers one question: which contracts are costing you money right now? Most physician groups have never asked this question systematically. The audit has three parts.
Inventory and triage your contracts
Gather every active payer contract into one place. Many groups store contracts across filing cabinets, email inboxes, and the memories of long-tenured staff. Until every agreement is centralized, you cannot evaluate the portfolio.
Once centralized, rank your payers by revenue contribution. Your top three payers typically represent 50-70% of collections. These contracts get priority. Flag any contract that has not been reviewed in two or more years for immediate attention.
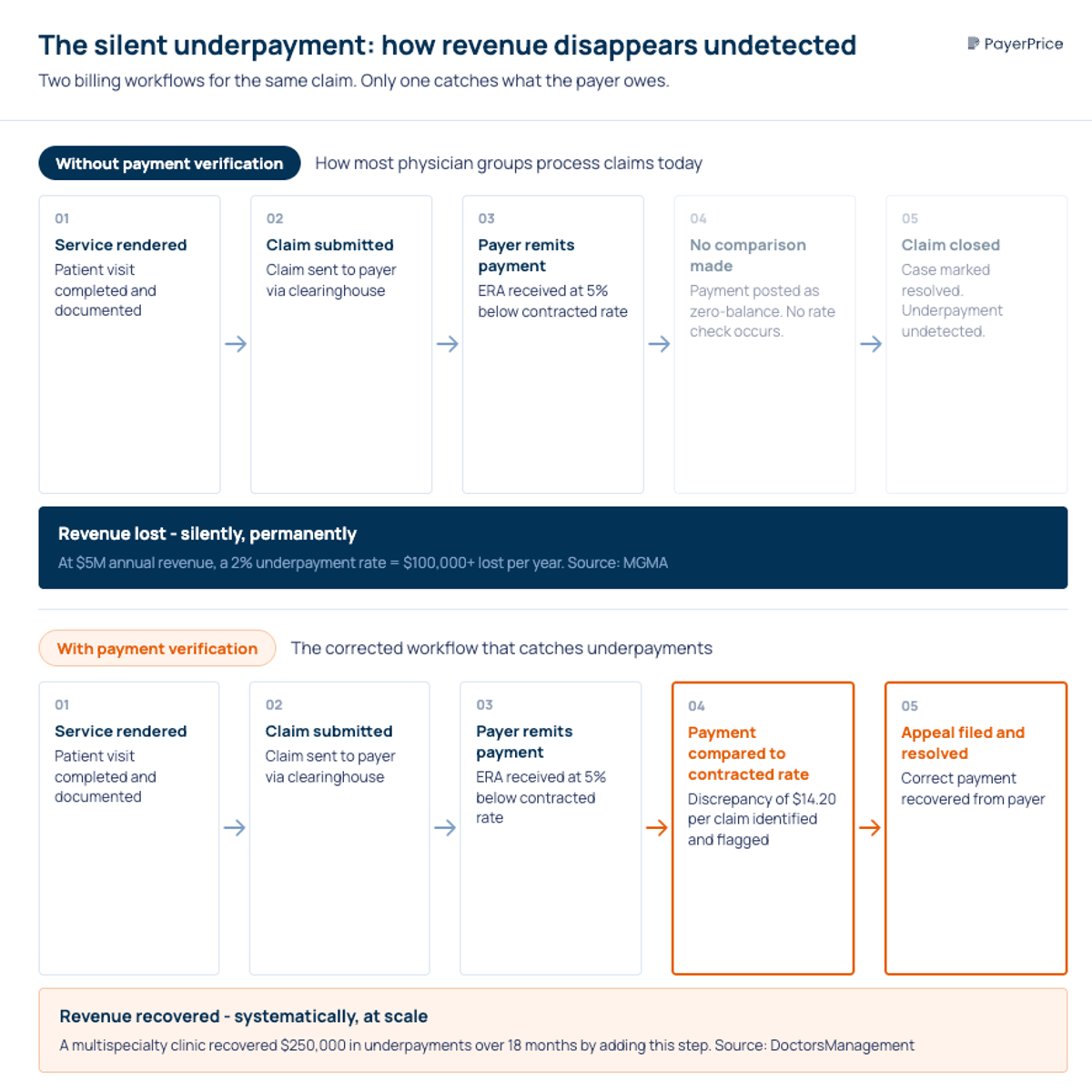
Detect silent underpayments
Silent underpayments are the biggest invisible leak in a physician group's revenue cycle. They happen when a payer remits less than the contracted allowable, but the billing system posts it as a fully resolved claim.
"Very few systems, and even fewer billing workflows, include a step where the posted payment is compared against the amount the payer was contractually obligated to pay."
- Matt Basham, Associate Management Consultant, DoctorsManagement [8]
To detect underpayments, you need to compare actual remittance amounts against your contracted fee schedules at the CPT code level. This means loading your contracted rates into a system that can match them against ERA (Electronic Remittance Advice) data. Manual spot-checking works for a sample, but systematic comparison across all claims is the only way to find patterns.
A multispecialty clinic case study documented by DoctorsManagement recovered $250,000 in underpayments over 18 months simply by comparing posted payments to contracted rates [8]. The underpayments had been occurring for years without detection.
Decode the "3% illusion"
A payer offers a 3% rate increase. Your team celebrates. But six months later, revenue has barely moved. What happened?
"If you take the word that it's a 3 percent increase, it might not be to revenue. Simply because of where the increases are happening on the fee schedule."
- Mark Schroeder, Aroris Healthcare
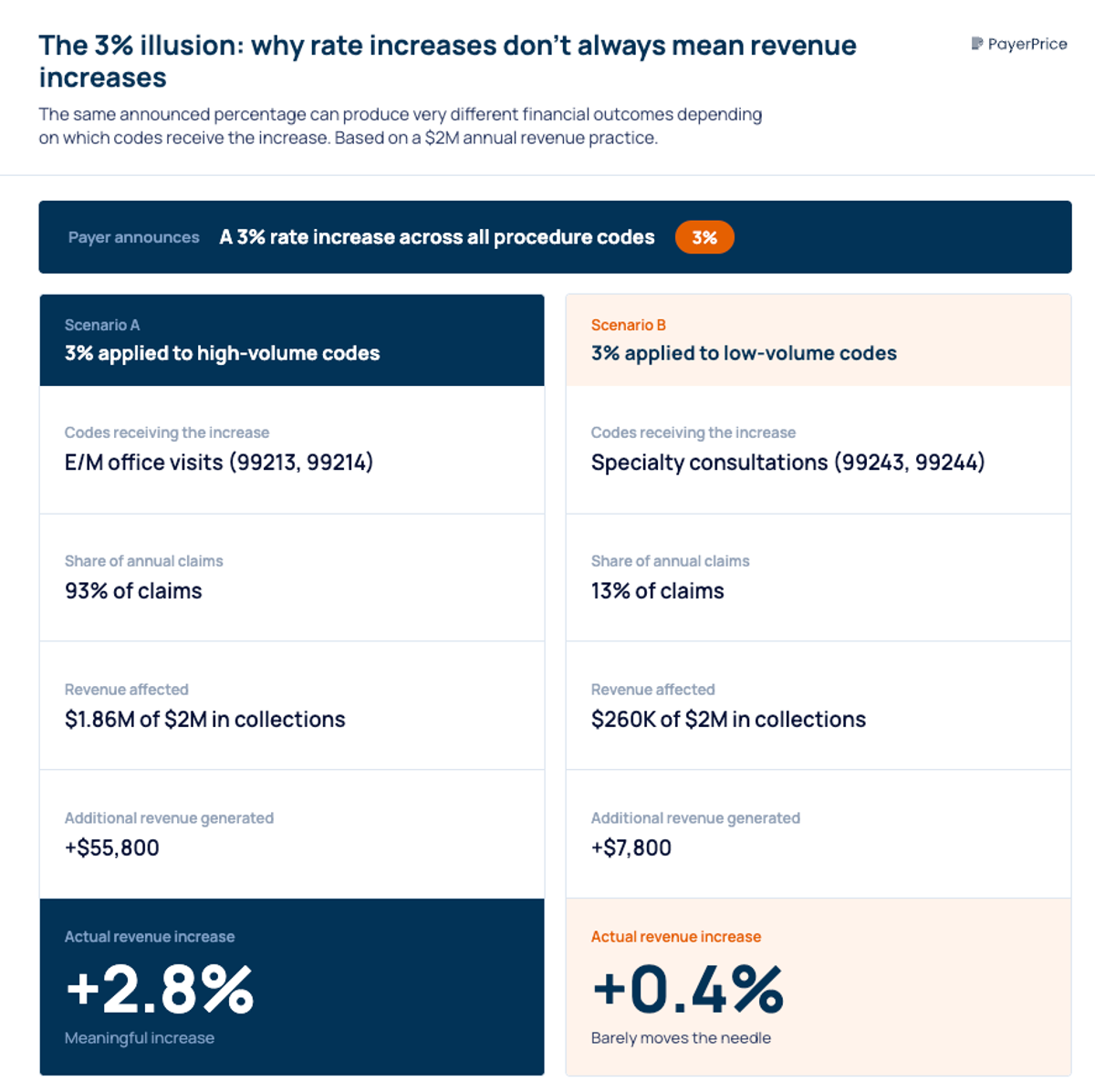
Payers apply rate increases strategically. A 3% increase concentrated on low-volume procedure codes (codes your group bills a few times per month) delivers almost no revenue impact. Meanwhile, your highest-volume codes, the E/M visits and procedures that drive 70% of collections, stay flat.
To evaluate a rate increase accurately, weight it by your actual claim volume. Multiply the rate change for each CPT code by the number of times you billed that code in the past 12 months. The sum is your real revenue impact, not the headline percentage.
This code-level analysis often reveals a gap between promised and actual value. Schroeder estimates that physician groups can be 15% behind market rates without knowing it.
That raises a critical question: how do you know what "market" looks like?
How to benchmark your rates against market data
Benchmarking answers the question every physician group needs answered before negotiation: are your rates competitive, and by how much do they lag? Until recently, this question was nearly impossible to answer. Payers had detailed internal databases of every rate they paid every provider. Physician groups had no equivalent.
"No one really wants to show their cards. Payers are not really transparent when they tell you what their medical necessity criteria are going to be. You have to stumble through it."
- Brad Gingerich, VP of Payer Strategy, Ensemble Health Partners [9]
That information asymmetry is starting to narrow. The Transparency in Coverage (TiC) rule, effective since July 2022, requires commercial payers to publish machine-readable files of their negotiated rates. These files contain the actual rates payers pay providers in your market, by CPT code, for every in-network contract.
The problem is access. According to an MGMA Stat poll from December 2025, only 18% of medical groups use TiC data in negotiations. The remaining 82% cite technical complexity, file size (individual files can exceed 100 GB), and lack of tools to parse the data.
For physician groups that can access this data, either through benchmarking platforms or analytics tools that parse TiC files, the negotiation dynamic changes. You can walk into a conversation with a payer and say: "Your competitor pays 112% of Medicare for this code. You pay 94%. Here's the data." That is a fundamentally different conversation than "We'd like a raise."
Other benchmarking sources that strengthen your position include Medicare fee schedules adjusted for your geographic practice cost index, MGMA DataDive peer comparisons, and FAIR Health databases covering 493 geographic regions.
The combination of transparency data and internal audit findings gives you the evidence base for negotiation.
How to negotiate payer contracts when you have limited leverage
Physician groups have more leverage than they realize, but it comes from data and preparation, not size. The conventional wisdom that only large health systems can negotiate effectively is wrong. It is also self-fulfilling: groups that believe they have no power don't negotiate, which means they never discover the leverage they actually hold.
Understand your value to the payer
Payers face increasing pressure to maintain adequate provider networks. According to KFF, Medicare Advantage enrollees have access to only 48% of the physicians available to traditional Medicare beneficiaries. Over the past three years, separations between MA plans and health systems have increased 66%, according to FTI Consulting.
Network adequacy rules require payers to maintain specific provider-to-member ratios by specialty and geography. If your group provides specialty services or covers an underserved geographic area, you fill a regulatory need the payer cannot ignore.
Start by documenting your patient volume by payer, your quality scores, and your geographic coverage. These three factors determine your practical leverage.
Build your case with data
Two frameworks make your proposal concrete rather than aspirational.
The first is a cost-per-RVU analysis: divide your total operating costs by your total RVUs to get your cost per RVU. If a payer's reimbursement falls below this number, you are losing money on every encounter with their members. That is a fact, not a request.
The second is a "hassle factor" analysis. Calculate each payer's prior authorization rate, first-submission denial rate, and appeal rejection rate. According to the 2026 Physicians Practice Payer Scorecard, 84% of practices are completing more prior authorizations than the prior year. If a payer requires prior auth on 30% of your claims, that administrative cost belongs in the negotiation.
"Is the juice worth the squeeze? And if it's not worth the squeeze, how do we tell the payer this? Because payers oftentimes don't understand the administrative burden components."
- Doral Jacobsen, CEO of Prosper Beyond
Watch for contract traps
Three contract provisions consistently hurt physician groups that overlook them.
Unilateral amendment clauses allow payers to change reimbursement terms mid-contract without your consent. The language is rarely explicit. Instead of stating "we will change rates mid-year," the contract uses vague phrasing like "terms subject to periodic review" or "provider agrees to comply with payer's current policies as amended." According to Medical Economics, unilateral amendments are one of the most common payer tactics.
Recoupment provisions give payers the right to claw back payments through post-payment audits, sometimes years after the original claim. These "payment integrity" programs have expanded significantly and represent an emerging financial threat to physician practices.
Auto-renewal clauses lock you into existing terms if you miss a notification window, which is often 90-120 days before expiration. Missing this window means another year at current rates with no opportunity to renegotiate.
Evaluate whether staying in-network is still viable
Some payer relationships cost more than they generate. If a payer's reimbursement falls below your cost per RVU, their denial rate exceeds 15%, and their prior auth burden consumes significant staff hours, the math points toward termination.
This is the option no one wants to discuss. But according to FTI Consulting data, provider-payer separations have increased 66% over three years [12]. Physician groups that are willing to walk away, when the data supports it, often find that payers return with better offers rather than lose network coverage.
How to monitor payer performance after signing
A signed contract is the beginning of payer contract management, not the end. The most common mistake physician groups make is treating negotiation as a one-time event, then filing the contract and forgetting it until renewal.
Ongoing monitoring requires tracking four metrics per payer, quarterly at minimum.
- Denial rate by payer. According to MGMA, 48% of medical group leaders say denials and appeals are their biggest revenue cycle leak [1]. Track first-pass denial rates and appeal success rates separately for each payer.
- Payment accuracy. Compare actual payments against contracted rates at the CPT code level. This is the silent underpayment detection from your initial audit, running as an ongoing process.
- Days to payment. Payers that consistently pay at 45-60 days instead of 30 create real cash flow costs. Track this and raise it in mid-contract performance reviews.
- Administrative burden. Count prior authorization requests, documentation demands, and staff hours per payer. This is your hassle factor, and it changes over time as payers adjust their policies.
Set calendar reminders for contract renewal windows. The notification deadline is often 90-120 days before expiration. According to Doral Jacobsen, "Once you conclude a negotiation, you need to identify the next time you should start it". The best practice is to begin preparation 12-18 months before contract expiration.
From contract neglect to revenue recovery
Physician groups lose revenue to payer contracts not because negotiation is impossible, but because contract management gets deprioritized beneath a hundred other operational fires. The four-step system, audit, benchmark, negotiate, monitor, turns a reactive process into a repeatable one.
Start with the audit. Pull every payer contract into one place. Rank them by revenue. Run a sample comparison of posted payments against contracted rates for your top three payers. If you find a gap, and most groups do, you have the evidence to justify investing in the rest of the process.
The Medwave case study puts a number on what is at stake: a 45-provider group practice that had not renegotiated contracts in over six years recovered $820,000 in additional annual revenue after a systematic review and renegotiation [16]. The contracts were not dramatically unfair. They were simply neglected.
That is the real cost of inaction, not a single bad deal, but years of small losses compounding silently across every claim, every payer, every day.
Share this article
Help spread the knowledge by sharing with others
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Related Articles
Continue exploring healthcare transparency and compliance topics
Underpayment Detection for Physician Groups: How to Find the Revenue Your Payers Owe You
Physician groups lose 5-7% of net revenue to payer underpayments hidden in zero-balance claims. Learn how to detect patterns and recover what you're owed.
How to Use TiC Data to Negotiate Better Payer Contracts: A Guide for Physician Groups
Learn how physician groups can use Transparency in Coverage negotiated rate data to benchmark rates, build payer-ready analyses, and win contract increases.
How to Model a Payer Contract: A Provider's Guide
See how providers model payer contracts against real claims to catch a money-losing deal before signing. Formulas, a worked example, and a 5-step method.