Payer Contracting: Why Most Healthcare Contracts Are Underperforming - and How Consultants Fix Them
Payer contracting is the backbone of how healthcare providers get paid for treating insured patients. These agreements spell out reimbursement rates, which services are covered, and set benchmarks that can seriously affect a provider's financial stability.


Cameron Fletcher
Head of Growth at PayerPrice
Most healthcare providers in the healthcare industry have contracts they have not reviewed in years. Those contracts auto-renew with flat rate increases while operating costs rise 5–8% annually, making it crucial to reassess payer contracting in healthcare.
A Boston Consulting Group study found that health systems need a 5–8% annual rate increase across all health plans to break even by 2027. Most contracts do not come close to that.
This article is written for payer contracting consultants : experienced practitioners who negotiate and manage payer contracts on behalf of hospitals, medical groups, ASCs, and post-acute providers.
It covers the structural problem behind underperforming contracts, the three forms of leverage that shift negotiations, and a practical execution sequence from audit to post-signature monitoring to ensure compliance in payer contracting in healthcare.
Why Most Payer Contracts Are Already Underperforming
Most payer contracts underperform because they were negotiated once and never revisited.
Many managed care contracts contain evergreen provisions : automatic renewal clauses that extend the agreement annually with no action required. Some include a fixed escalator of 2–3% to help ensure compliance and address rising costs in payer contracting.
Many include none at all. For a practice billing $10 million per year with rates 5% below the regional market, that gap is $500,000 in annual lost revenue : and none of it appears as a denial that triggers a billing flag.
Brad Gingerich, VP of Payer Strategy at Ensemble Health Partners, described this in a Healthcare de Jure podcast interview:
"I came to find, early in my career, that many of these contracts were neglected; there was never really a focus on them."
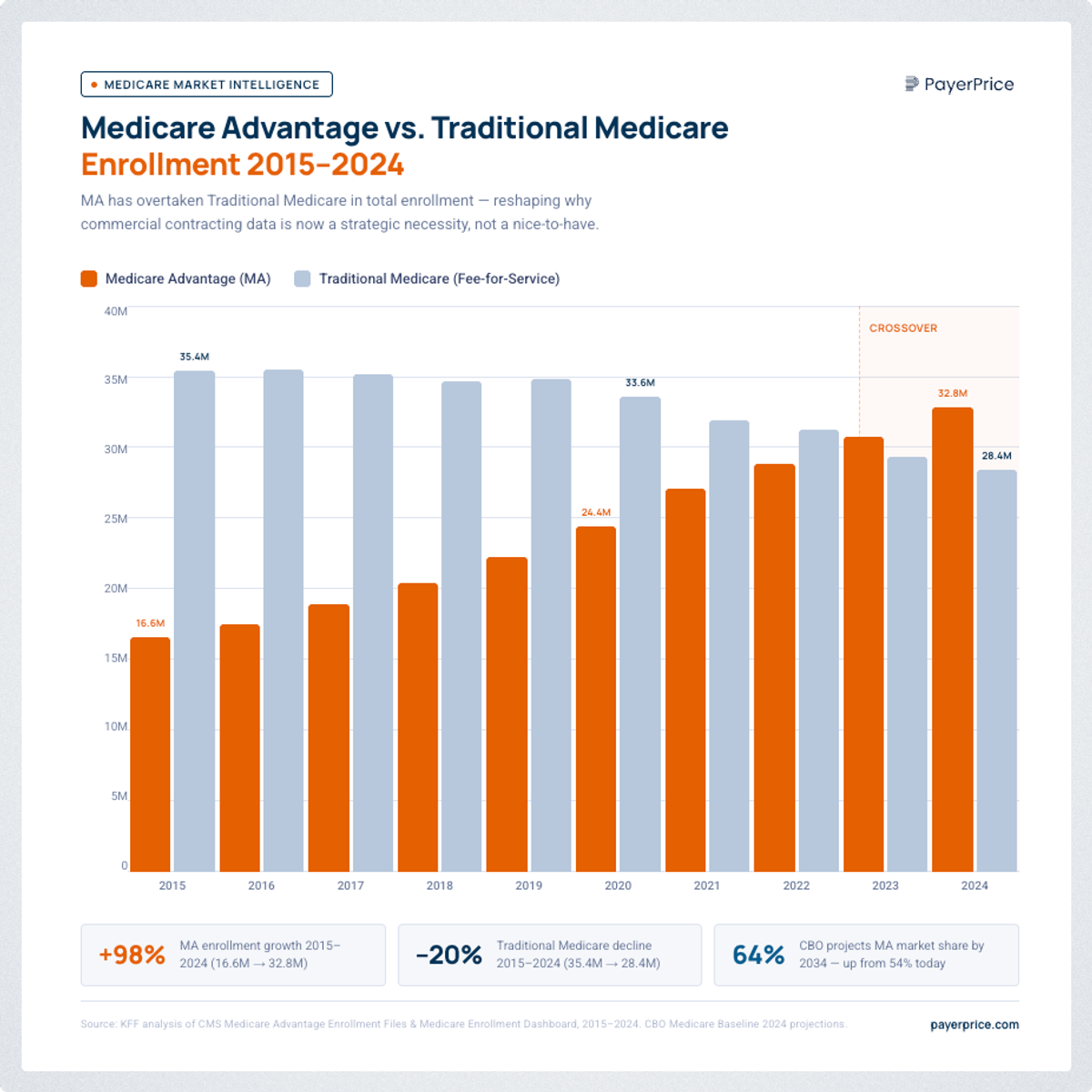
The neglect problem is compounded by a structural shift. By 2025, 54% of all Medicare beneficiaries were enrolled in Medicare Advantage (MA) plans, according to CMS data analyzed by KFF.
Unlike traditional Medicare : which pays on a fixed, publicly available fee schedule : MA plans pay through negotiated commercial contracts. Rural hospitals currently receive approximately 90.6% of traditional Medicare rates from MA plans on a cost basis, according to the American Hospital Association. Fifty percent of rural hospitals now operate at a loss.
Every additional Medicare beneficiary who enrolls in an MA plan converts a fixed, predictable revenue stream into a negotiated commercial contract. Providers who treated managed care as secondary five years ago can no longer afford to do so.
What a Payer Contract Actually Controls
Payer contracting is the process of negotiating and managing the agreements between healthcare providers and insurers that determine how services are reimbursed.
The rate is only one element in the broader context of payer contracting in healthcare and its impact on patient care. A payer contract governs reimbursement rates by CPT and HCPCS code, the payment timeline for Clean claims are essential for ensuring compliance and reducing costs in the payer contracting process., claims submission rules and documentation requirements, prior authorization criteria, dispute resolution procedures, and termination notice periods.
The language governing adjudication timelines and dispute procedures determines whether the rates in the contract translate into actual revenue. A contract with a favorable rate but a 45-day clean-claim processing window and no late-payment penalty gives the payer flexibility that erodes the headline rate over time.
According to MGMA data, underpayments account for 3–5% of contracted revenue annually for most practices, impacting their ability to ensure compliance and deliver quality patient care. A claim paid at 94% of the contracted rate looks like a paid claim in most billing systems. Detecting systematic underpayment requires running actual payments against contract terms at the code level : a step most providers skip entirely.
The Three Forms of Leverage in Payer Contracting
Leverage in payer contracting comes from three sources: data, network access, and the internal payer champion.
1. Data Leverage
Data leverage is the ability to make a specific, quantified ask backed by claims history to ensure compliance and improve payer contracting. Claims history is vital for ensuring compliance and optimizing payer contracting in healthcare. and regional benchmarks.
Before any negotiation, assemble the client's top 20–30 CPT codes by volume for the relevant payer, the current contracted rate for each, the regional market rate drawn from price transparency data This directly impacts the annual revenue and the ability to deliver quality patient care by closing the gap. This converts the rate request from a general ask into a line-by-line comparison.
Price transparency regulations now require hospitals and insurers to publish negotiated rates, which means a provider can look up what a competitor receives from the same payer for the same service. That data converts the negotiation from "what we think we deserve" to "what the market actually pays."
The practical complication: most clients arrive without this data organized for the contracting process. Reconstructing CPT utilization reports and compiling fee schedules from PDF contracts is usually the first deliverable in a consulting engagement : and it consistently takes longer than expected.
Ready to benchmark other commercial payer rate?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
2. Network Scarcity Leverage
Network scarcity leverage comes from selectively managing which payers a provider contracts with.
Gingerich described the cost of doing the opposite:
"Health systems were giving away network access : a provider might have contracts with every payer without creating scarcity around that notion. Collectively, this open access to a provider's network pushed reimbursement rates down."
Network scarcity leverage requires the provider to be genuinely willing to go out of network if rates are inadequate. MA plan members choose their plan partly based on which providers are in network, so a credible threat to leave creates real pressure on the payer. The leverage available depends on market position : a specialty group with dominant local market share has more of it than a primary care practice in an oversupplied market. Identifying whether a client has network scarcity leverage is an early-stage assessment in every engagement.
3. Champion Leverage
Champion leverage is the ability to identify and enable a specific person inside the payer organization who has both the motivation and authority to move the contract forward in the contracting process.
Payer organizations require sign-off from network management, legal, actuarial, and compliance to finalize contracts with insurance companies. No single person approves a contract unilaterally : but someone inside the organization has a stake in getting yours executed within the healthcare industry.
Marta Bralic Kerns, CEO of Pomelo Care, described this in an Out-of-Pocket Health interview: even after finding a champion who responded with "oh my God, thank God you're here," it still took three months to close the contract.
Without a champion in the contracting in healthcare process, the contracting process stalls indefinitely, affecting the ability to deliver quality patient care. Her team ran nine sales calls per week specifically to find these people faster.
Once a champion is identified, the consultant's job is to make their internal approval path frictionless : having the contract template ready, knowing whether the client is contracting as a provider or a vendor, and giving the champion a specific next step rather than leaving the process undefined.
What Consultants Do Differently From Internal Teams
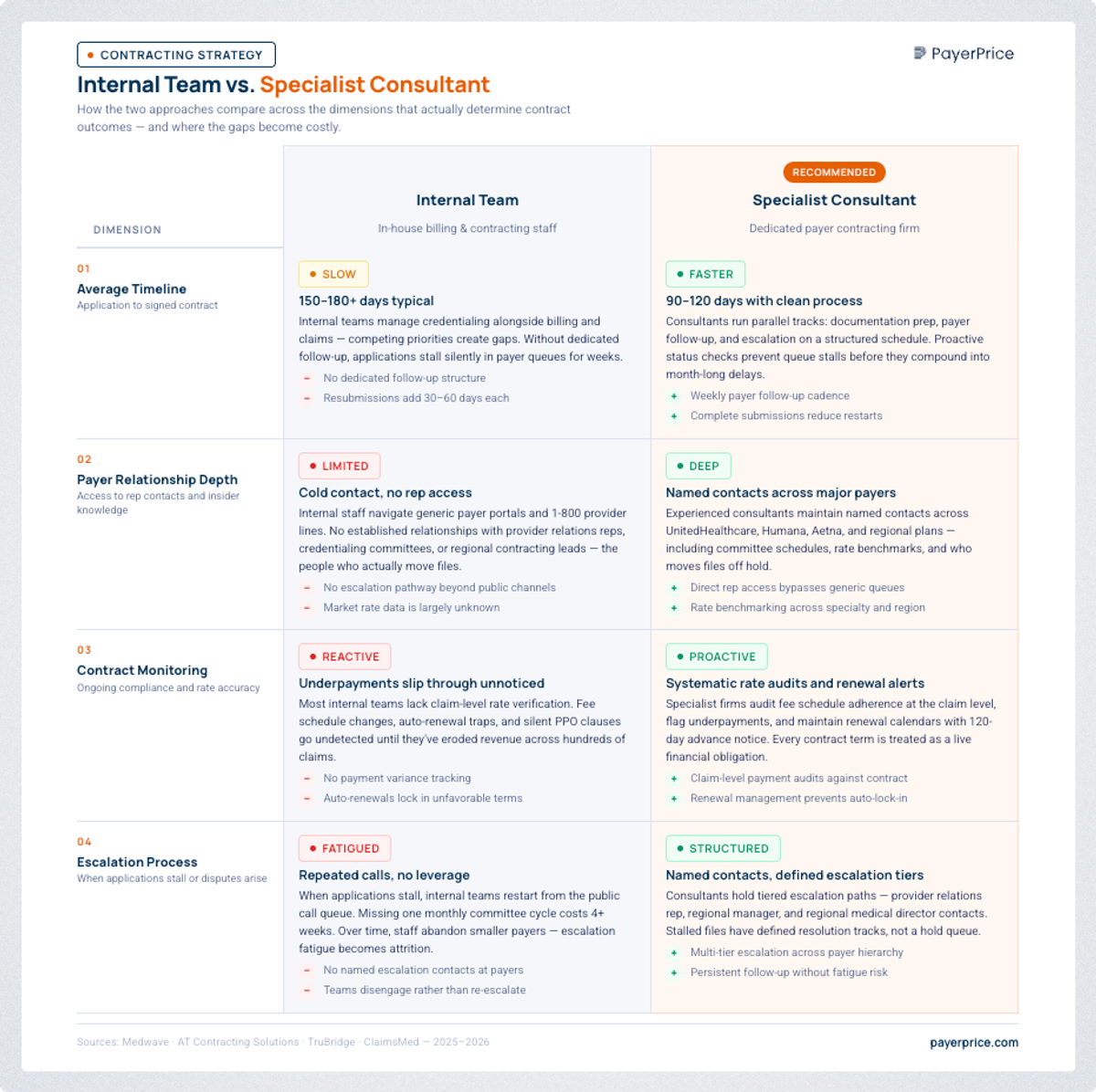
A specialist consultant reduces the contracting timeline, improves final rates, and catches post-signature payment errors that internal staff miss.
Four differences that determine outcomes:
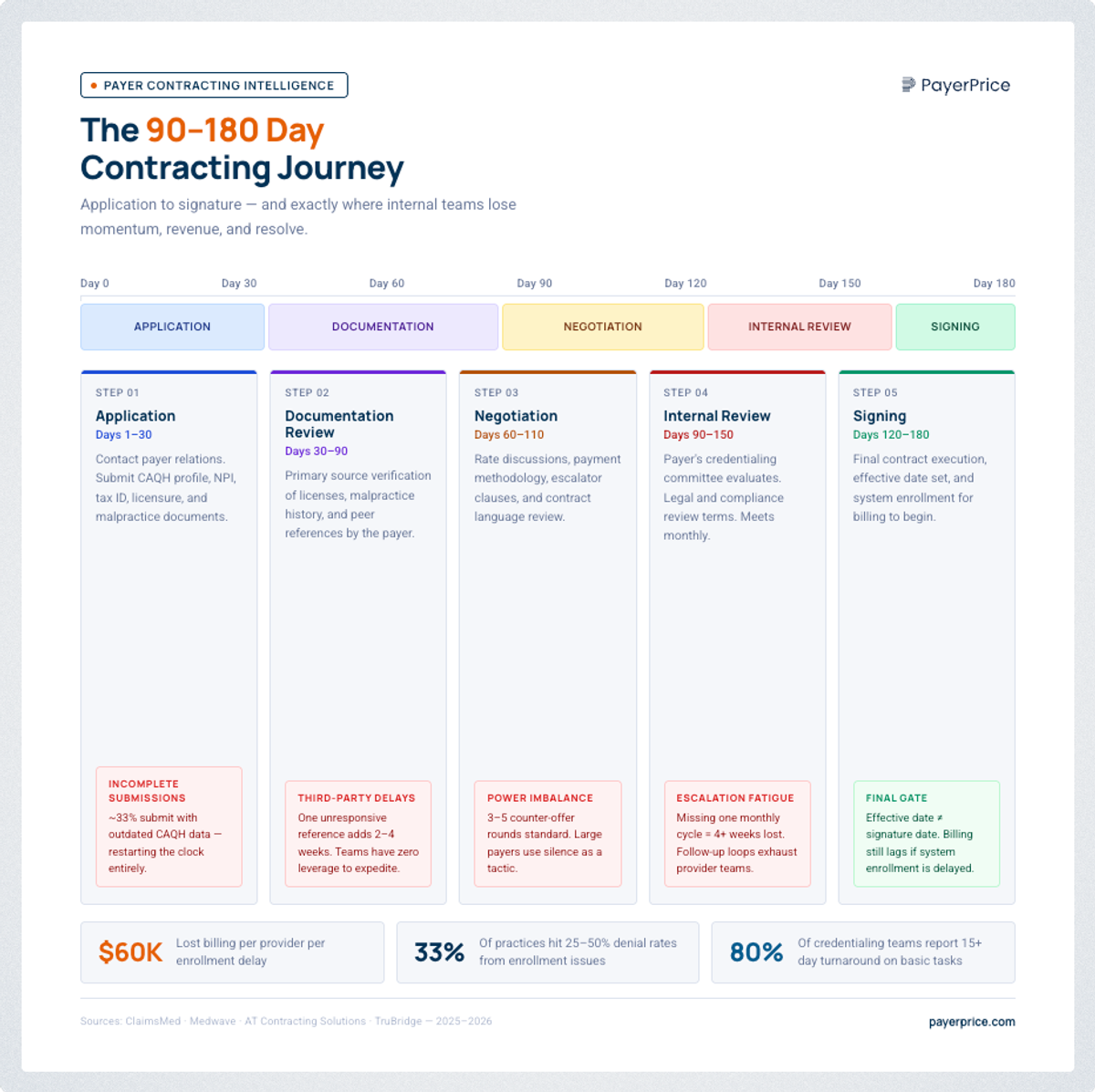
Timeline: With a specialist, negotiating a commercial contract typically takes 90–180 days from application to execution. Internal teams without established payer contacts regularly exceed 180 days : often reaching 12 months : due to incomplete submissions and escalation fatigue: payers ignoring renegotiation requests is a deliberate tactic to get providers to accept the status quo.
Payer relationships: A consultant working across 10–20 active engagements maintains ongoing relationships with network development staff at major commercial plans. An internal staff member calling a payer cold has no relationship capital and no knowledge of which internal contact has authority.
Pattern recognition in contract management: A consultant who has negotiated the same structure with the same payer multiple times knows where the real rate flexibility is and which contract clauses are negotiable in practice. Internal teams that negotiate once every few years do not develop best practices in contract management.
Post-signature monitoring: Payers make implementation errors after a rate change : continuing to apply old fee schedules, misclassifying CPT codes, failing to update adjudication systems. A consultant runs actual claims payments against new contract terms for 90–120 days post-signature and initiates disputes before variances accumulate. Most internal teams move to the next priority after signing and never detect the problem.
Payer Contracting Strategy: Step by Step
Effective payer contracting follows seven steps from portfolio audit to post-signature monitoring.
Step 1 : Audit the contract portfolio. Identify every active payer agreement, its auto-renewal date, current rates for the top CPT codes, and whether rate escalators have actually been applied in the context of value-based care. Most organizations find contracts no one was tracking and renewal dates that have already passed.
Step 2 : Benchmark current rates for medical services. Compare current contracted rates against regional market rates using price transparency data. This produces a priority list: which payers are furthest below market, and what is the annual revenue impact of closing the gap.
Step 3 : Prioritize by impact and timing. Focus on the highest-revenue-impact payers where a natural renegotiation window exists in the next 12 months to improve contract management. Not all contracts are worth pursuing simultaneously.
Step 4 : Build the negotiation case. Assemble CPT volume data, current rates, regional market rates, and the delta expressed in annual revenue impact. The goal is a specific proposal: "Our current rate for CPT 99213 is $98. The regional median is $117. We are requesting $115." This shifts the conversation from percentages to specific codes.
Step 5 : Identify the right payer contact. Network development managers are the right entry point for new contracts. For renegotiations, provider relations may own the relationship but not the rate decision. Use existing relationships and referrals to reach someone with actual approval authority rather than entering through the standard customer service channel.
Step 6 : Execute with a defined timeline. Submit the proposal with a specific response deadline and a target execution date to streamline the contracting process. Address the full contract during negotiation : not just the headline rate. Adjudication timeline language, prior authorization requirements, and dispute resolution windows can erode the value of a favorable rate over the life of the agreement.
Step 7 : Monitor claims for 90–120 days post-signature to ensure compliance with the new payor contract. Run actual payments against new contract terms at the code level to assess the effectiveness of the contracting process. Identify any claims paid below the new contracted rate and initiate the dispute process immediately to ensure compliance and reduce costs. Underpayments that go undetected in this period establish a payment pattern that requires a formal appeal to correct rather than a simple system fix.
Conclusion
Payer contracting in healthcare is the most actionable revenue lever available to most healthcare organizations in the healthcare industry to ensure compliance and deliver quality patient care. With Medicare Advantage now covering over half of Medicare beneficiaries and MA plans reimbursing below cost in many markets, the gap between what providers are paid and what they need to operate is widening.
Closing that gap requires the same three levers across every engagement: data to make specific, defensible asks; network access managed deliberately to create real pressure; and a champion inside the payer who can move the contract through approval. The consultants who execute this consistently audit contracts that have been auto-renewing for years, benchmark rates against a market that has moved, and monitor payments after signing to catch the implementation errors that quietly erode the rate increase just negotiated.
As Gingerich stated: "One of the last remaining opportunities to actually drive revenue into a health system is those negotiated contracts you have with payers to ensure compliance and deliver quality patient care." For most organizations, the contracts in place today do not reflect what the market supports, hindering their ability to ensure compliance and deliver quality patient care. Closing that gap starts with a complete picture of what those contracts actually say.
Share this article
Help spread the knowledge by sharing with others
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Related Articles
Continue exploring healthcare transparency and compliance topics
Underpayment Detection for Physician Groups: How to Find the Revenue Your Payers Owe You
Physician groups lose 5-7% of net revenue to payer underpayments hidden in zero-balance claims. Learn how to detect patterns and recover what you're owed.
How to Use TiC Data to Negotiate Better Payer Contracts: A Guide for Physician Groups
Learn how physician groups can use Transparency in Coverage negotiated rate data to benchmark rates, build payer-ready analyses, and win contract increases.
How to Model a Payer Contract: A Provider's Guide
See how providers model payer contracts against real claims to catch a money-losing deal before signing. Formulas, a worked example, and a 5-step method.