Ophthalmology & Retina Coding Guide: Billing & Coding
2026 ophthalmology and retina coding guide for the retina practice. CPT codes, billing and coding, diagnostic imaging, cataract, ophthalmic reimbursement.


Cameron Fletcher
Head of Growth at PayerPrice
Ophthalmology and retina coding guide: 2026 billing and coding playbook for RCM consultants
You just signed an ophthalmology or retina practice as a new client. The billing manager hands you last quarter's denial reports and says the practice is leaking somewhere they cannot find. You have two weeks to tell them where the money is, in dollars.
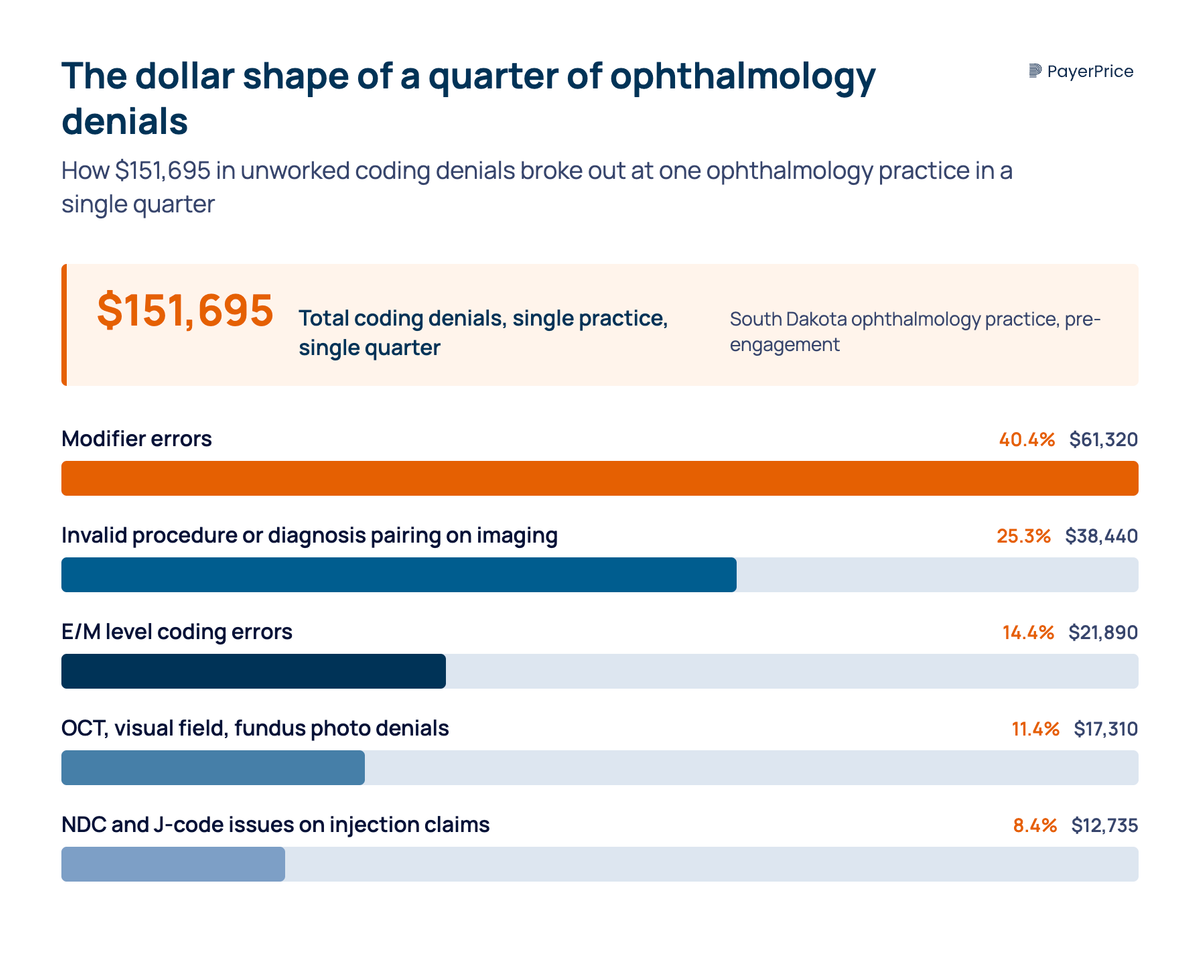
According to a South Dakota ophthalmology case study published by MBW RCM, one quarter of unworked coding denials totaled $151,695: modifier errors, invalid CPT-to-ICD-10 pairing on diagnostic imaging, E&M level errors, OCT and fundus photography denials, and NDC plus J-code issues on injection claims. That is the dollar shape of a typical engagement.
This ophthalmology and retina coding guide covers the ophthalmology CPT codes that matter, the 2026 changes that drive denial volume, and a 90-day diagnostic playbook for RCM consultants.
What makes ophthalmology and retina billing and coding different
Six structural features make ophthalmology and retina billing and coding behave differently from any other specialty in your book of business, and the consultant who recognizes them in week one closes the engagement faster than one who treats it like primary care.
- Two parallel office visit code families. Ophthalmology is the only specialty where the eye visit codes (CPT codes 92002-92014) and the 99xxx E&M codes are interchangeable for many payers. The election is a margin lever most general consultants miss.
- Drug inventory as a balance sheet item. Anti-VEGF drugs (Eylea, Lucentis, Vabysmo, Avastin, Eylea HD, Syfovre, Izervay) carry per-vial costs in the four-figure range. According to MBW RCM, retina drug inventory represents 35 to 50 percent of practice operating cost.
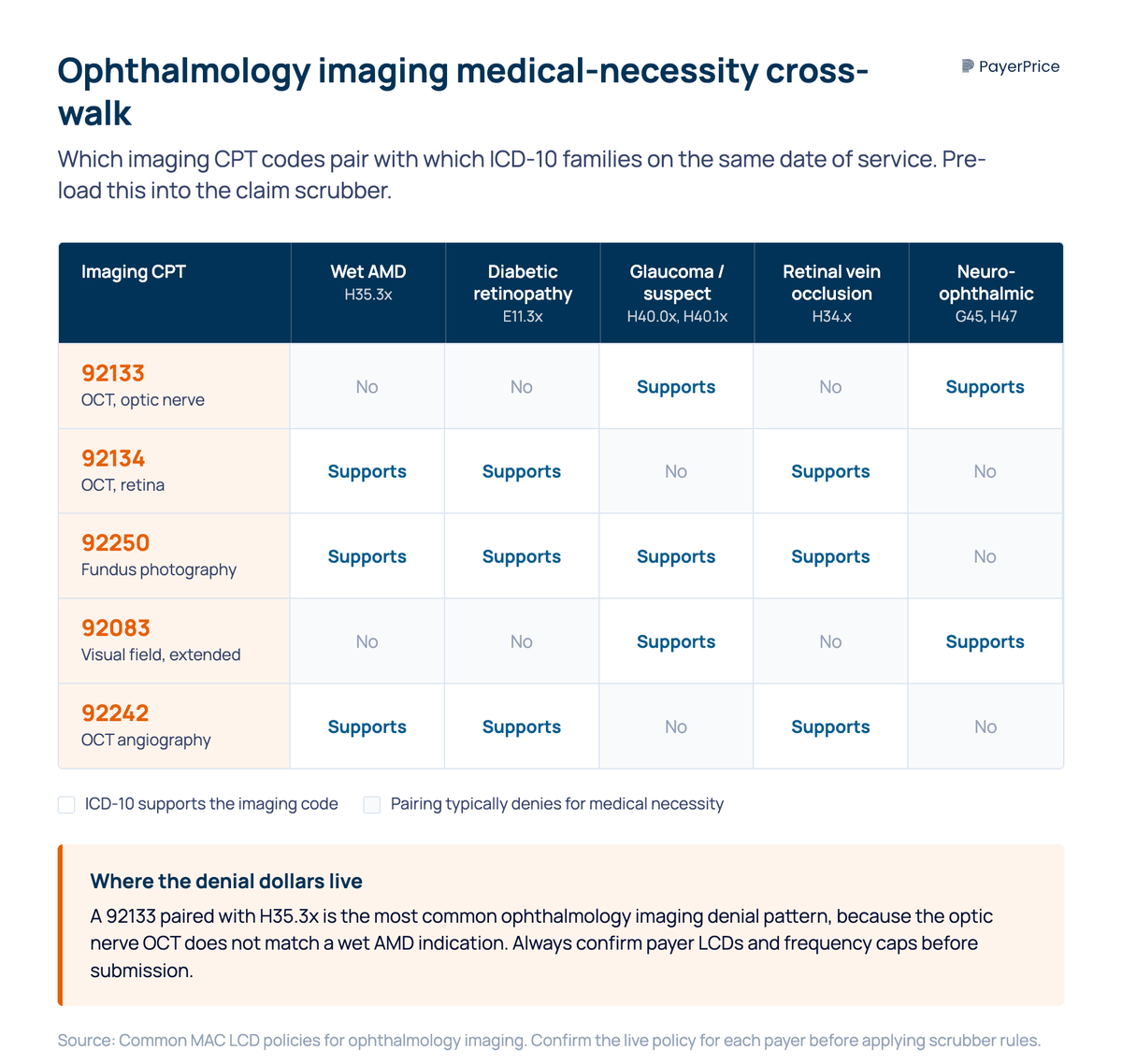
- Diagnostic imaging as a daily, frequency-edited workflow. OCT 92133 and 92134, fundus photography 92250, visual field 92083, and OCT angiography 92242 each have MAC LCD frequency rules and ICD-10 medical necessity pairings.
- Bilateral procedure rules that do not generalize. RT, LT, and 50 modifier behavior on diagnostic imaging and procedures varies by code description and payer.
- A payer audit posture pointed at intravitreal injection plus same-day E&M. CMS Targeted Probe and Educate audits are active on this pairing per Corcoran Consulting Group's Ophthalmology Reimbursed podcast.
- Buy-and-bill cash flow risk. The retina practice fronts five-figure drug inventory before claims adjudicate.
Eye exams and office visit codes (CPT codes 92002-92014)
The single highest-leverage office visit decision in ophthalmology is the election between an eye visit code and an E&M code, and a consultant who audits the mix usually finds the practice defaulting to one family and leaving money on the table. Both code families capture the service provided during the office visit; the dollars and documentation requirements differ.
The two families:
- Eye visit codes. Code 92002 is the intermediate new-patient eye exam, 92004 the comprehensive new-patient exam, 92012 the established-patient intermediate, 92014 the established-patient comprehensive. Intermediate codes require 3 to 11 of the 12 American Academy of Ophthalmology exam elements; comprehensive codes require all 12.
- Evaluation and Management (E&M) codes. 99202 to 99205 for new patient, 99212 to 99215 for established patient. Per the American Medical Association's 2021 revision to Current Procedural Terminology (CPT), level is selected by medical decision making (MDM) or total time.
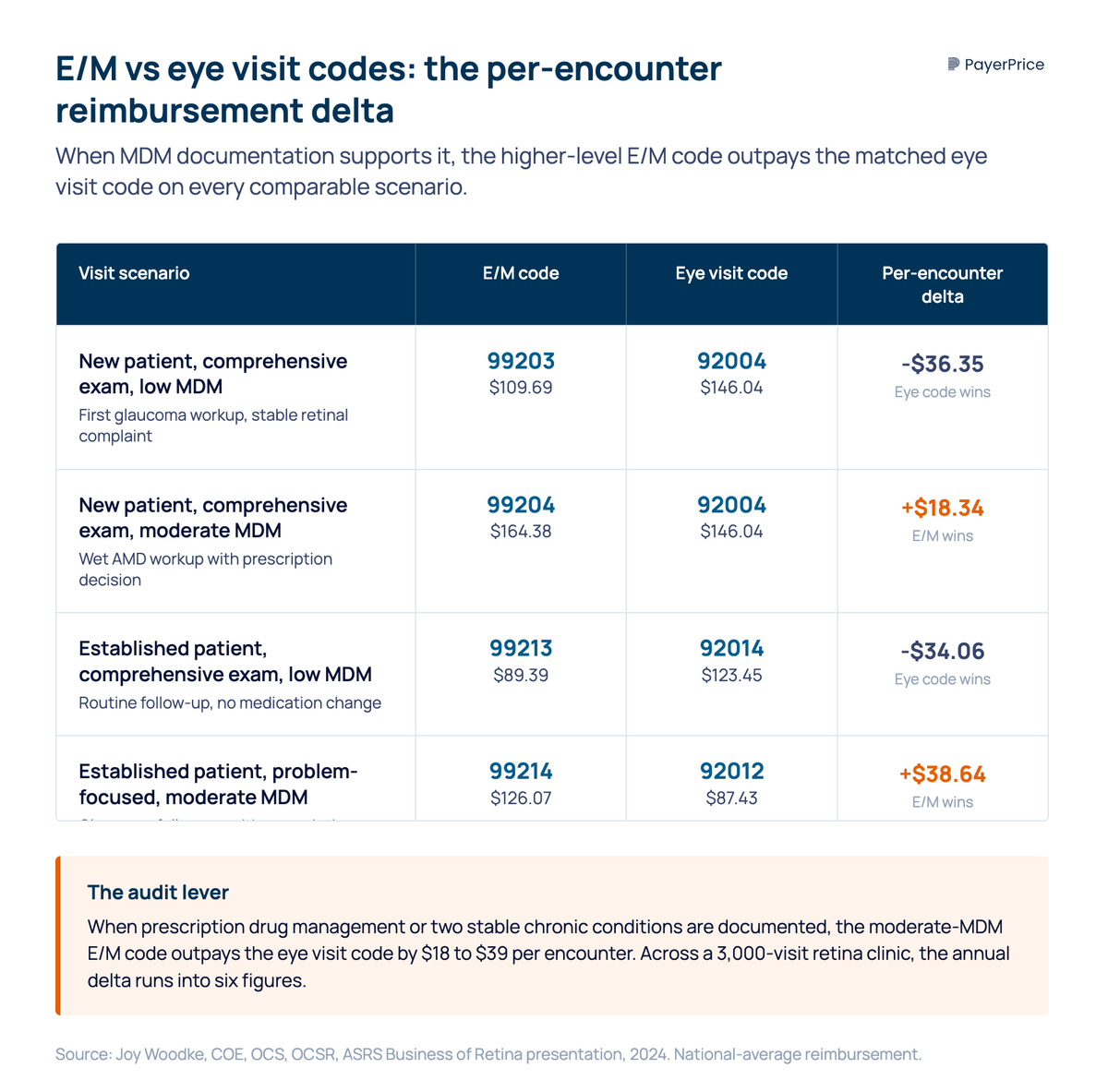
The pairwise reimbursement deltas matter. According to Joy Woodke, COE, OCS, OCSR (Director of Coding and Reimbursement at the American Academy of Ophthalmology), an established patient with a comprehensive exam and moderate MDM bills at 99214 ($126.07) versus 92012 ($87.43), a delta of more than $38 per encounter. A new patient with comprehensive exam and moderate MDM bills at 99204 ($164.38) versus 92004 ($146.04). Across a year of follow-ups in a high-volume retina practice, the election compounds.
"Understanding both eye and E/M codes allows the ophthalmologist to maximize reimbursement by choosing the code that most accurately represents the level of service."
- Brittney Irwin, COT, CPC-A, CEP, BSM Consulting
ICD-10 codes specificity governs everything downstream. Diabetic retinopathy (E11.3xx, including diabetic macular edema and proliferative diabetic retinopathy), age-related macular degeneration (H35.3x), retinal detachment (H33.xx, including rhegmatogenous retinal detachment), glaucoma (H40.xx), and retinal vein occlusion (H34.xx) are the high-volume diagnosis codes. Specificity supports the medical necessity edits on the diagnostic imaging codes in the next section.
Diagnostic imaging CPT codes: 92133, 92134, 92250, and 92083
Diagnostic imaging denials are the second largest dollar category in the typical ophthalmology engagement, and the root cause is almost always a frequency edit or unsupported ICD-10 to CPT pairing. The MBW South Dakota case attributed $17,310 to imaging denials and another $38,440 to invalid CPT-diagnosis pairing largely on imaging.
The CPT code stack the consultant pre-loads into the scrubber:
- CPT code 92133. OCT, optic nerve. Glaucoma workup and follow-up.
- CPT code 92134. OCT, retina. The workhorse for age-related macular degeneration, diabetic macular edema, and most retinal conditions affecting the macula.
- CPT code 92250. Fundus photography. Documentation and serial monitoring.
- CPT code 92083. Extended visual field examination. Glaucoma and neuro-ophthalmic indications.
- CPT code 92242. OCT angiography. Diabetic and macula indications, growing volume.
Each specific code maps to a defined diagnostic test, and coding information published by each MAC governs frequency caps. MAC LCDs cap 92133 at one to two per year for stable glaucoma; 92134 frequency varies by retinal indication and payer. National Correct Coding Initiative (NCCI) edits add another layer.
Medical necessity drives the other half of denials. Each diagnostic imaging code requires an ICD-10 on the same date that supports the diagnostic tests billed. AMD (H35.3x) supports 92134 and 92250; glaucoma (H40.0x) supports 92133 and 92083; diabetic retinopathy (E11.3x) supports 92134, 92250, and 92242. A claim pairing 92133 with H35.3x denies because the optic nerve OCT is not the diagnostic test indicated by AMD.
CPT codes 92133 and 92134 are bilateral by description, so RT for the right eye and LT for the left eye are rarely needed; modifier 50 sometimes triggers payer-specific reductions.
Surgical CPT codes: retina, cataract, and ophthalmic procedures
Retina surgery bundling rules are the most counterintuitive in the specialty, and a multi-specialty RCM consultant inheriting a surgical practice will not have seen these patterns elsewhere. Three same-session pairings appear repeatedly in denied claims.
According to Elizabeth Cifers, MBA, MSW, CHC, CPC (owner, Elizabeth Cifers Consulting), the canonical same-eye, same-session bundling traps in retina surgery are:
- Pars plana vitrectomy plus intraocular lens (IOL) reposition. IOL reposition carries a "separate procedure" designation, not separately billable.
- Pars plana vitrectomy plus intravitreal injection. The injection is a "separate procedure" not billable in the same vitrectomy session.
- Pars plana vitrectomy plus posterior segment laser. Laser bundles into the vitrectomy code.
Ophthalmology CPT codes for retina surgery: vitrectomy 67036 through 67043 (combined with epiretinal membrane peel, focal endolaser, or gas tamponade); retinal detachment repair 67110 (pneumatic retinopexy), 67107 (scleral buckle through the sclera), 67108 (vitrectomy-based); retinal cryopexy 67101; intravitreal injection 67028 (XXX global, separately billable from same-day E&M when modifier 25 is supported).
Cataract surgery: 66984 (routine extracapsular cataract removal with phacoemulsification and IOL implantation), 66982 (complex), 66987 (drug-eluting intraocular lens). Pre-operative biometry covers corneal measurements through 76519 (A-scan) and 92136 (IOL Master). The anterior and posterior segments each carry their own code stack.
Glaucoma surgical procedures: 65855 (laser trabeculoplasty), 66170 (trabeculectomy), 66174 (canaloplasty), 66183 (anterior segment aqueous drainage device, MIGS shunt).
Most retina surgery carries a 090-day global; modifier 24 covers an unrelated office visit in the global period, modifier 78 covers an unplanned OR return, modifier 58 covers a planned staged procedure. Modifier 25 carries the highest dollar exposure of any modifier in retina because it sits on top of the highest-volume procedure.
Anti-VEGF injection billing, J-codes, and reimbursement
Anti-VEGF injection billing is the single largest dollar exposure in retina, and the consultant who connects the J-code mechanics on the claim line to the buy-and-bill economics fixes problems an in-house biller cannot see. A 2 to 3 percent rate variance on a single drug line generates six-figure annual losses at most retina volumes.
The 2026 J-code stack for major intravitreal agents:
- J0178. Aflibercept 2 mg (Eylea, Regeneron).
- J0177. Aflibercept 8 mg (Eylea HD, Regeneron).
- J2778. Ranibizumab 0.1 mg (Lucentis, Genentech / Roche).
- J9035. Bevacizumab 10 mg (Avastin, Genentech / Roche).
- J3398. Faricimab-svoa 6 mg (Vabysmo, Genentech / Roche).
- J2781. Pegcetacoplan 1 mg (Syfovre, Apellis), geographic atrophy.
- J2782. Avacincaptad pegol 0.1 mg (Izervay, Astellas), geographic atrophy.
Proper coding for anti-VEGF injections requires three claim-line rules. Units bill by the HCPCS dosage description, not vial size. The National Drug Code (NDC) is required on the claim line for most commercial payers. Modifier JZ (mandated since July 2023 for single-use vials with no waste) and modifier JW (documented waste) close out wastage discipline. Coding experts at Corcoran Consulting Group flag medical billing for retina drug claims as the highest-risk category in the specialty.
"Mistakes made in selecting the drug code, factoring the units to bill, linking the correct diagnosis, and/or addressing drug wastage can be expensive."
- Joy Woodke, COE, OCS, OCSR, AAO Director of Coding and Reimbursement
Buy-and-bill cash flow is the structural risk. Medicare pays separately payable Part B drugs at ASP plus 6 percent (cross-check current rates with the Medicare fee schedule lookup). Commercial contracts vary, and NOC drugs without a permanent HCPCS billing code often pay as a percentage of billed fee. The retina practice fronts five-figure drug inventory before claims adjudicate.
Practice management for RCM consultants: the leaks, MIPS, and the 90-day playbook
The five reimbursement leaks an RCM consultant audits on every ophthalmology and retina engagement are modifier 25 on intravitreal injection days, diagnostic imaging medical necessity, NDC and J-code discipline, contract underpayment on anti-VEGF lines, and E&M downcoding by payer. Each leak resolves to a measurable KPI shift.
Ranked by dollar exposure:
- Modifier 25 on intravitreal injection days. CMS TPE audits target this exact pairing.
- Diagnostic imaging medical necessity and frequency. Cross-walk ICD-10 to imaging code at the scrubber so 92133 paired with H35.3x never submits.
- NDC, J-code, JW, and JZ discipline. Five-figure quarterly exposure on a single missed JZ.
- Silent contract underpayment on anti-VEGF lines. A 2 to 3 percent rate variance on a J0178 line generates six figures annually.
- E&M downcoding. Humana and other commercial payers convert level 4 E&M visits to level 3.
According to Lindsay Stratton at Eye Med Management Solutions, a single denied retinal procedure costs $3,000 to $5,000 in lost revenue plus $25 to $50 in rework.
The Merit-Based Incentive Payment System (MIPS) sits on top of these leaks. Ophthalmology MIPS quality measures cover diabetic retinopathy screening, AMD documentation, and primary open-angle glaucoma optic nerve evaluation. A clean coding operation feeds clean MIPS reporting; a leaky one drags MIPS scores with reimbursement.
The 90-day audit sequence:
- Week 1. Pull denial reports by CPT and reason code, payer mix, and top 20-CPT contracted-versus-paid variance.
- Week 2. Audit modifier 25 documentation on the last 100 CPT 67028 claims with same-day E&M.
- Week 4. Audit NDC, JZ, and JW discipline on those 100 injection claims.
- Week 6. Audit the diagnostic imaging ICD-10 to CPT scrubber rules.
- Week 8. Reconcile the top 10 commercial fee schedules against current Medicare ASP for J0178 and J3398. Price transparency data confirms what competing practices are paid for the same J-codes.
- Week 12. Deliver the recovery report and lock scrubber rule changes.
What the practice expects on your first invoice
The essential CPT codes for retina practice (67028, 92134, 92133, 92250, 92083, J0178, J3398) and the eye conditions they map to (wet AMD, diabetic macular edema, glaucoma, geographic atrophy) sit at the center of the audit.
Three actions take the engagement to a measured KPI shift inside 30 days. First, audit modifier 25 documentation on the last 100 CPT 67028 claims; most practices fail at least 15 percent of the sample. Second, pull the diagnostic imaging denial report by ICD-10 to CPT pairing and write the top three corrections into the claim scrubber. Third, reconcile the top 10 commercial payer fee schedules against current Medicare ASP for J0178 (Eylea) and J3398 (Vabysmo); a 2 to 3 percent variance generates a six-figure annual underpayment the billing system will not flag.
Underpayment recovery on high-cost drug lines is where rate-benchmarking platforms like PayerPrice sit behind the coding function and convert the consultant's audit into recovered cash.
Share this article
Help spread the knowledge by sharing with others
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Related Articles
Continue exploring healthcare transparency and compliance topics
How to Model a Payer Contract: A Provider's Guide
See how providers model payer contracts against real claims to catch a money-losing deal before signing. Formulas, a worked example, and a 5-step method.
How to Run Payer Contract Analytics (Physician Group Guide)
Stop signing stealth pay cuts. This guide shows physician groups how to benchmark rates, recover underpayments, and run payer contract analytics in-house.
How to Contract With Insurance Companies (Without a Bad Rate)
How to contract with insurance companies as a provider: the credentialing steps, the contract clauses to check, and how to tell if your rate is fair before you sign.