Underpayment Detection for Physician Groups: How to Find the Revenue Your Payers Owe You
Physician groups lose 5-7% of net revenue to payer underpayments that hide inside zero-balance claims. This guide shows how to detect them systematically and turn the findings into contract negotiation leverage.


Cameron Fletcher
Head of Growth at PayerPrice
Your payer sends a payment. Your billing system posts it. The claim shows a zero balance. Everyone moves on.
But zero balance does not mean the payer paid the correct amount. It means your system reconciled what it received against what the payer reported as allowed. If the payer applied the wrong fee schedule, bundled two procedures that should have been paid separately, or downcoded your E/M level, the shortfall disappears into a contractual adjustment that no one audits.
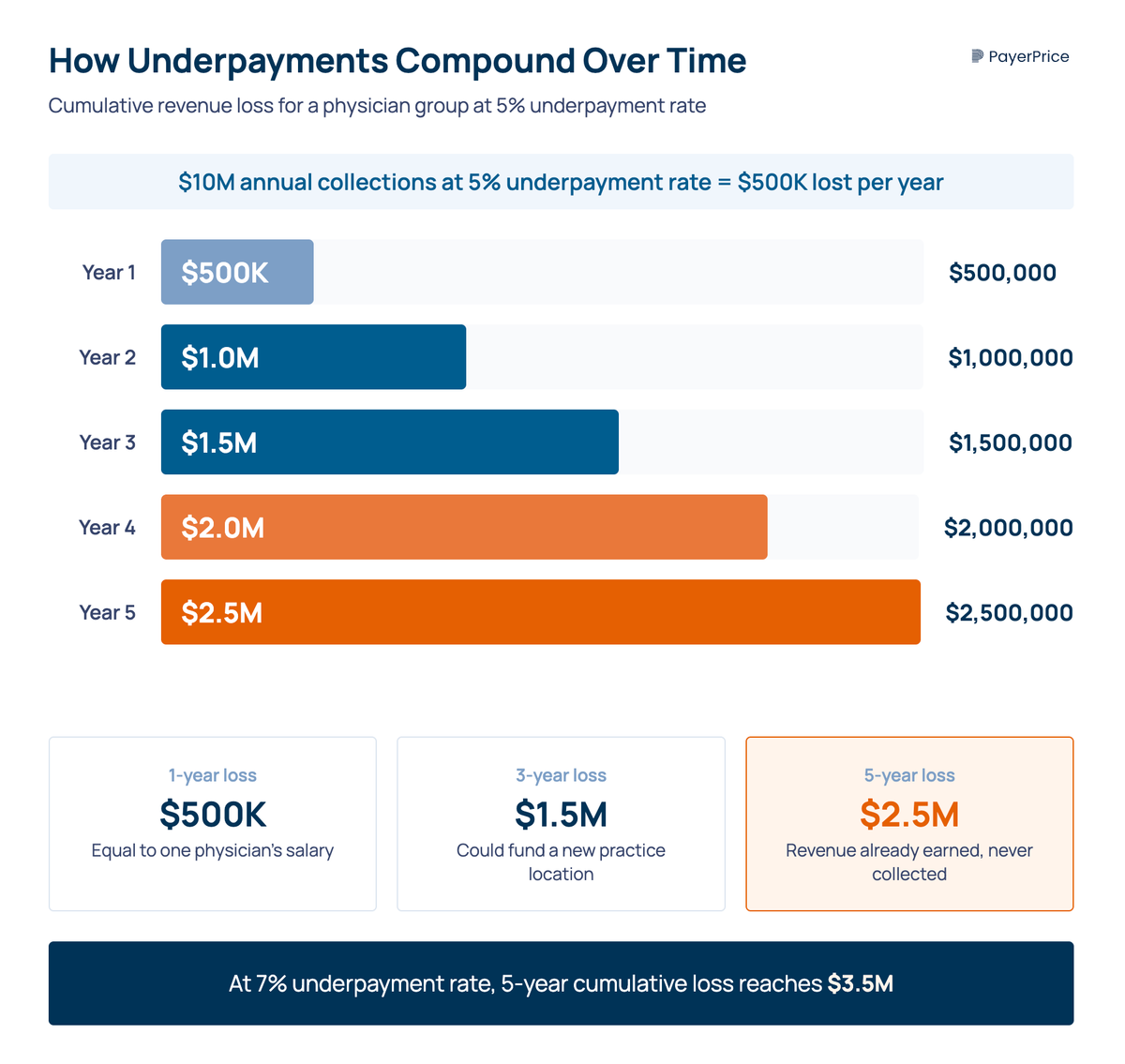
According to MGMA, small-to-midsize physician groups face underpayment rates of 5-7% of net revenue. For a group collecting $10 million annually, that is $500,000-$700,000 in revenue already earned, for services already rendered, that payers keep. Over five years, the losses compound past $2.5 million.
This guide covers how physician groups can detect underpayments without enterprise software, identify the most common patterns payers use to underpay professional fees, and turn every underpayment finding into data for your next contract negotiation.
Why physician groups lose more to underpayments than hospitals do
Physician groups face higher underpayment rates than large health systems because they lack dedicated contract management staff, track fee schedules manually, and have less bargaining power with payers.
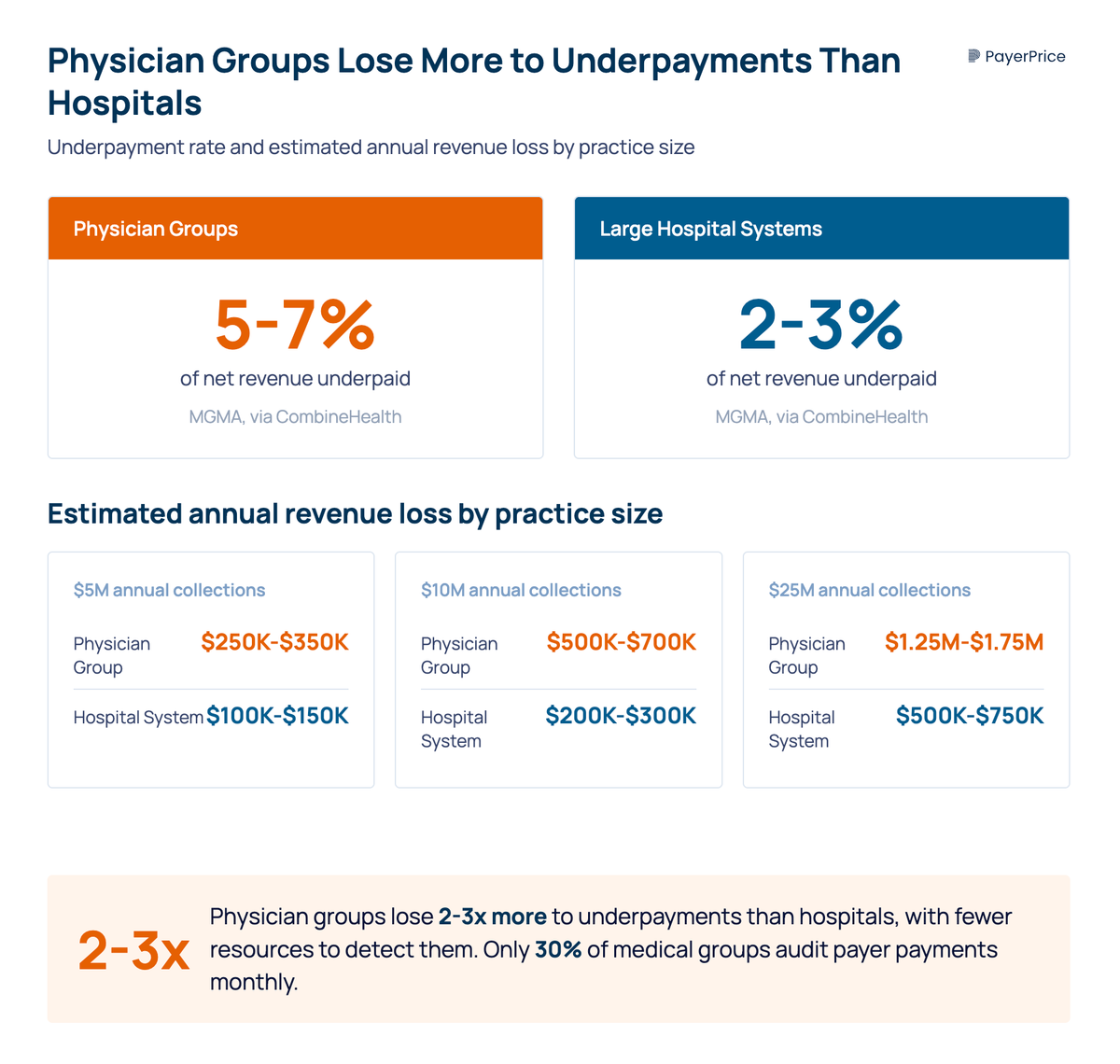
According to CombineHealth (citing MGMA data), small-to-midsize physician groups experience underpayment rates of 5-7%, compared to 2-3% for large hospital systems.
The gap comes down to resources. A 200-bed hospital has a revenue integrity department, contract management software, and analysts who audit payments full-time. A 15-provider physician group has a billing team of three to five people who handle everything from eligibility verification to collections. Underpayment auditing falls to the bottom of the priority list, if it makes the list at all.
"The billing team is focused on getting claims out the door and collecting on aging receivables. The practice administrator is managing a hundred other priorities. And the physicians, who ultimately bear the financial impact of underpayments, are typically unaware the problem exists."
- Matt Basham, Associate Management Consultant, DoctorsManagement
According to an MGMA Stat poll, only 30% of medical group practices audit payer payments monthly. Another 18% audit quarterly. The remaining 52% audit annually, sporadically, or not at all. One respondent put it plainly: "It's ridiculous how often payments are incorrect."
The financial pressure is compounding. According to MGMA's 2025 Medicare data, physician practice operating costs increased over 63% from 2013-2022, while the Medicare conversion factor increased by only 1.7% over the same period. Losing an additional 5-7% on commercial claims to undetected underpayments turns a tight margin into an unsustainable one.
That raises a basic question: if underpayments are this common, why do they go unnoticed?
What underpayment detection means (and why zero-balance claims hide the problem)
Underpayment detection is the process of comparing what a payer actually paid on a claim against what your contract says they owe. The gap between those two numbers is the underpayment. The reason physician groups miss it: underpayments do not trigger alerts in your practice management system. They settle quietly as zero-balance transactions.
Here is how it works. Your practice bills CPT 99215 for an established patient visit. Your contract with Payer X says the allowed amount is $185. Payer X remits $162. Your PM system posts the $162 payment, writes off $23 as a contractual adjustment, and closes the claim at zero balance. No flag. No notification. No one reviews the $23 shortfall because the claim looks resolved.
"When a payer remits a payment that is three, five, or fifteen percent below the contracted allowable, the claim settles quietly into the system as a zero-balance transaction. Nobody disputes it because nobody knows it happened."
- Matt Basham, DoctorsManagement
Two categories of underpayments matter for detection. Idiosyncratic underpayments are one-off processing errors: a claim keyed incorrectly, a fee schedule loaded wrong for a single code. These are random and low-value individually. Systematic underpayments are consistent patterns where a payer underpays the same code, modifier, or service type across hundreds or thousands of claims. Systematic underpayments are where the real revenue loss accumulates, and they are the ones worth building a detection process around.
Knowing that the problem exists is one thing. Knowing exactly which payer behaviors cause it gives your billing team something to look for.
The 5 most common underpayment patterns in physician groups
Professional fee underpayments follow predictable patterns that repeat across payers and specialties.
Recognizing these patterns turns underpayment detection from a claim-by-claim review into a targeted audit.
Here are the five patterns physician groups encounter most often:
1. E/M level downcoding
The payer reimburses at a lower E/M level than billed. You submit 99215; they pay the 99214 rate. According to the AMA, "payers are increasingly implementing E/M downcoding programs that inappropriately reduce payment for claims" and "doing so in ways that make it extremely difficult to identify in coding audits." According to a Karen Zupko & Associates white paper, by 2025, payers including UnitedHealthcare, Cigna, Aetna, and regional BCBS plans began using AI-driven automated downcoding as a routine cost-control strategy. For practices, revenue erosion from downcoding alone can reach six-figure annual losses.
2. Modifier bundling and denial
Payers ignore or incorrectly bundle modifier -25 (separate E/M on the same day as a procedure) and modifier -59/-XE (distinct procedural service). According to the OIG, 35% of Medicare claims with modifier -25 did not meet program requirements - and payers use this finding to justify blanket denials or reductions. According to MGMA, improper modifier handling leads to a 10-20% increase in claim denials.
3. Fee schedule drift
Your contract rate increased at renewal, but the payer's adjudication system still pays the old rate. This is common after auto-renewed contracts where rate adjustments take effect on paper but never get loaded into the payer's system. According to an MGMA poll, 33% of providers fail to review their contracts yearly, and 17% report never reviewing them. If you do not check, the payer has no incentive to correct the error.
4. Multi-procedure payment reductions applied incorrectly
When billing multiple procedures in the same session, payers apply reductions to the second and subsequent procedures. The standard Medicare reduction is 50% on the second procedure. Some commercial payers apply deeper reductions than the contract allows, or apply reductions to procedures that should be exempt.
5. Incorrect coordination of benefits
For patients with dual coverage, the primary payer sometimes shifts more of the allowed amount to the secondary payer or patient than the contract permits. The result: neither payer pays the full contracted amount, and your practice absorbs the difference.
Each of these patterns produces a specific signature on the ERA. Downcoding shows up as a lower-than-expected allowed amount on E/M codes. Modifier bundling appears as a $0 payment on the modifier-appended line. Fee schedule drift produces a consistent percentage shortfall across all claims from one payer. Once you know what to look for, you can build a detection process around these signals.
How to build an underpayment detection process without enterprise software
A quarterly payer audit that takes 2-4 hours per payer gives physician groups a systematic way to catch underpayments without purchasing contract management software. The process has five steps.
Step 1: Centralize your contract rate data
Create a single reference document - even a spreadsheet - listing each payer's contracted allowed amounts for your top 20-30 CPT codes by volume. Include E/M levels (99211-99215), your highest-volume procedures, and any codes with modifiers you bill frequently (-25, -59, -XE). If your contracts reference a percentage of Medicare, pull the current Medicare fee schedule rates and calculate the expected amounts. This step is where most practices stall. Do it once, update it when contracts renew, and every future audit becomes faster.
Step 2: Sample and compare
Pull a random sample of 50-100 paid claims per payer per quarter from your PM system. For each claim, compare the actual payment (from the ERA) to the expected payment (from your contract rate reference). Flag any variance above 2%. Sort the flagged claims by CPT code to see if the same codes keep appearing.
Step 3: Identify patterns
A single underpaid claim is a processing error. The same underpayment across 50 claims from the same payer on the same CPT code is systematic. Focus your attention on systematic patterns because they represent the largest recoverable revenue and the strongest evidence for disputes. For example, if Payer X consistently pays your 99215 at the 99214 rate, that is a downcoding pattern worth quantifying.
Step 4: Quantify the annual impact
Extrapolate your sample findings to estimate total annual underpayment per payer. If 12 out of 100 sampled claims from Payer X were underpaid by an average of $35, and Payer X processes 4,000 claims per year for your group, the estimated annual impact is $16,800 from that payer alone. Run this calculation for each payer. The aggregate number is your practice's total underpayment exposure.
Step 5: File disputes with documentation
Submit formal disputes for underpaid claims within the payer's filing deadline. Commercial payers typically allow 90-120 days from the date of payment; Medicare allows 120 days; Medicaid varies by state. Include the contract terms, ERA data, and pattern evidence in each dispute. Batch similar underpayments together - a dispute showing 200 claims with the same underpayment pattern is harder for a payer to dismiss than 200 individual disputes.
Detection alone recovers lost revenue. But the data from your audits also gives you something more valuable for the long term: leverage.
From detection to leverage: using underpayment data in payer contract negotiations
Every underpayment you detect is a data point for your next contract negotiation. Most physician groups treat underpayment recovery and contract negotiation as separate activities. Connecting them changes your position at the negotiation table from "we'd like higher rates" to "here is documented evidence that you are not paying the rates we already agreed to."
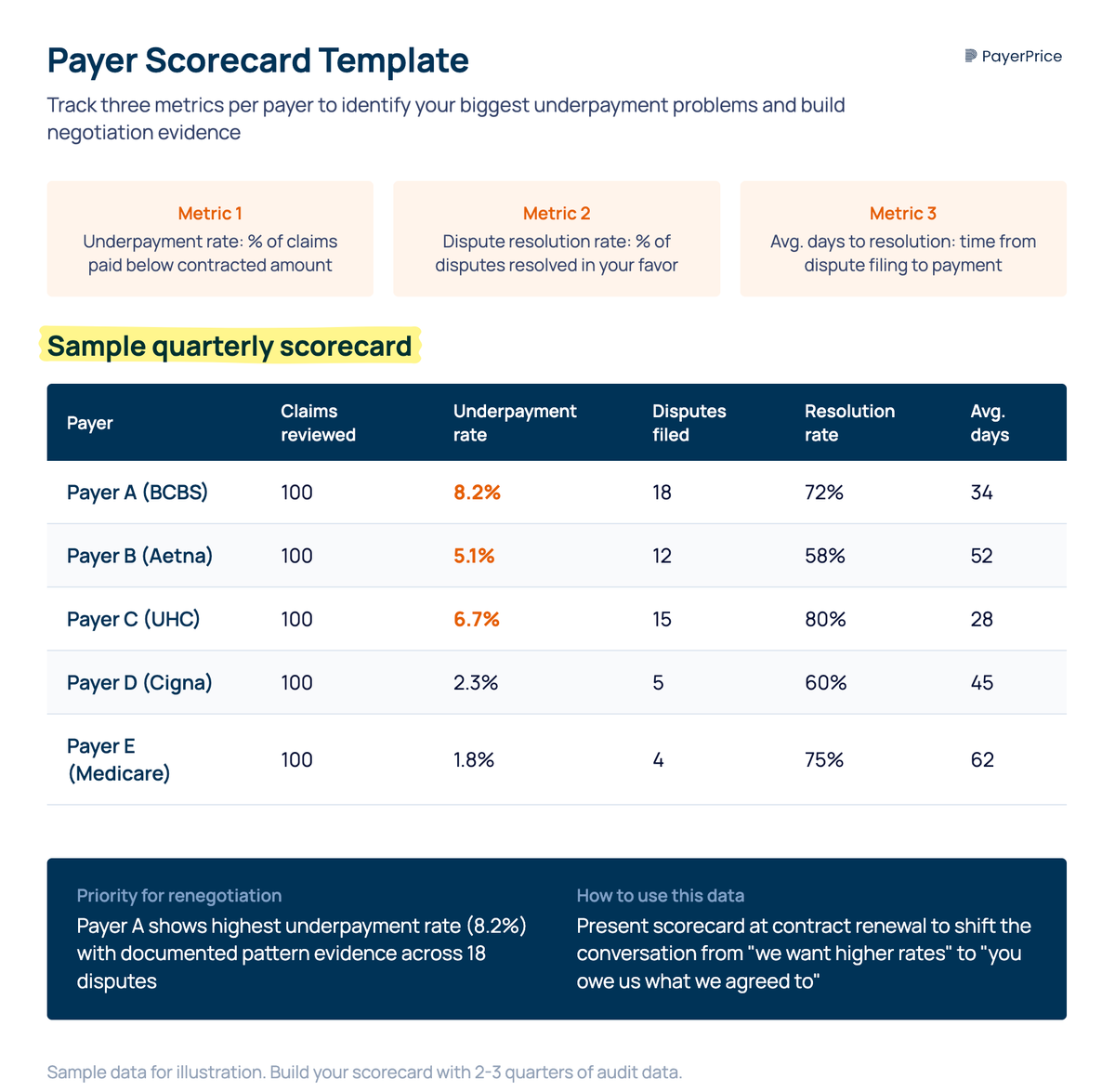
Build a payer scorecard that tracks three metrics per payer: underpayment rate (percentage of claims paid below contracted amount), dispute resolution rate (percentage of disputes resolved in your favor), and average days to resolution. After two or three quarters of data, this scorecard tells you which payers are your biggest problems and gives you evidence when you renegotiate.
According to QuickIntell, payers pay more accurately when they know a provider has automated detection in place. The deterrent effect is real: systematic monitoring signals to the payer that underpayments will be caught and disputed, which reduces future underpayment volume even before your next negotiation.
"Most payer contracts auto-renew. And most practices let them. Why? Because renegotiation feels intimidating. Because the data isn't readily available. Because people assume, 'We don't have leverage.'"
- Jill Arena, CEO, Health e Practices
Underpayment data removes the "data isn't readily available" barrier. If your audit shows that Payer X underpaid 8% of claims over the past year, totaling $45,000 in shortfalls, you walk into that negotiation with a specific, documented problem and a clear ask: pay what you already agreed to pay, and here is the evidence that you have not been.
If disputes and negotiations fail to resolve systematic underpayments, physician groups have additional options. Most states have prompt-pay laws that require payers to process clean claims within 30-45 days and pay interest on late or incorrect payments. Filing a complaint with your state insurance commissioner creates a formal record that can accelerate resolution.
Start with one payer and 50 claims
A physician group collecting $10 million annually and losing 5% to underpayments is losing $500,000 every year. Over five years, that is $2.5 million in revenue already earned that payers kept.
The minimum viable first step: pick your highest-volume commercial payer. Pull 50 recent paid claims. Compare each payment to your contracted rate. If you find a pattern, you have found revenue to recover and data to negotiate with. If every claim matches, move to the next payer.
Underpayment detection for physician groups is not about purchasing enterprise software or hiring a dedicated analyst. It is about building a repeatable quarterly process that treats paid claims with the same scrutiny your team already applies to denied claims. The revenue is already yours. The question is whether you are checking to make sure you received it.
Share this article
Help spread the knowledge by sharing with others
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Related Articles
Continue exploring healthcare transparency and compliance topics
How to Use TiC Data to Negotiate Better Payer Contracts: A Guide for Physician Groups
Learn how physician groups can use Transparency in Coverage negotiated rate data to benchmark rates, build payer-ready analyses, and win contract increases.
How to Model a Payer Contract: A Provider's Guide
See how providers model payer contracts against real claims to catch a money-losing deal before signing. Formulas, a worked example, and a 5-step method.
How to Run Payer Contract Analytics (Physician Group Guide)
Stop signing stealth pay cuts. This guide shows physician groups how to benchmark rates, recover underpayments, and run payer contract analytics in-house.