Value-Based Contract Guide for Physician Groups & Value-Based Care
Navigate value-based care contracts with our guide for physician groups. Learn about risk-sharing agreements, payer incentives, and real-world quality metrics.


Cameron Fletcher
Head of Growth at PayerPrice
A value-based contract proposal sits on your desk. The shared-savings split reads fair on the cover page, the quality metrics fill three appendices, and the payer's representative wants a signature before the quarter ends. You already sense the economics can go sideways, but the proposal does not tell you where.
According to a JAMA Health Forum research letter (2024), primary care physicians now manage a mean of ~57 unique quality metrics across ~8 value-based care contracts per year. Performance-year payment often lags that work by 18 to 20 months. One primary care physician interviewed for the Commonwealth Fund's focus-group study summed up the lived experience in a single line:
"Great on paper, impossible to implement in reality."
- Primary care physician, Mathematica and Commonwealth Fund focus-group study, 2024
Sign the wrong agreement and your group inherits the reporting burden, the 18-month cash-flow hole, and downside risk the payer priced into the margin. Reject a fair deal out of caution and you forfeit shared savings, quality bonuses, and a defensible position in next year's negotiation.
This playbook gives you a three-part framework to evaluate any value-based contract before you sign: a six-dimension readiness test that tells you whether your group can actually operate the contract, market-standard benchmarks for the terms payers will quote you, and a red-flag clause list with ten payer questions that turn a one-sided proposal into a fair one.
What value-based care contracts actually mean for a physician group
A value-based care contract ties a physician group's compensation to measurable cost, quality, and utilization outcomes for a defined patient population, instead of paying per claim under fee-for-service.
Value-based contracts in health care now span the entire health care system, from Medicare Advantage and Medicaid services administered by the Centers for Medicare and Medicaid Services to commercial plans and government programs.
The shift toward value-based payment models is driven by health policy efforts to tie care payment to quality and cost, not volume. The use of value-based contracts grew alongside rising health care spending, and interest in value-based contracts across care organizations, ACOs, and IPAs continues to climb as every health system searches for a workable cost curve. The increased use of value-based care contracts now shapes almost every commercial and Medicare renewal a physician group sees.
One disambiguation is worth making before you evaluate the proposal on your desk. The phrase "value-based contracting" is also used by pharmaceutical manufacturers to describe outcomes-based contracts in which rebates are tied to real-world patient outcomes. Novartis entered VBCs with Aetna and Cigna for Entresto, tying rebates to the observed frequency of hospitalization for heart failure. Harvard Pilgrim reached a similar outcomes-based contract with Amgen for a PCSK9 inhibitor, linking remuneration to measured outcomes in real-world populations, specifically LDL reduction. These pharma agreements turn on a formula that determines the net price of a drug, using ASC 606 revenue recognition, Medicaid Best Price accounting, and anti-kickback statute safe harbors. A closed formulary, clinical trials data, and real-world evidence sit behind the model, and the stated aim is improving health outcomes while containing total drug spend. Closed formularies, formulary-tier negotiations, and rebate clawbacks are the operational levers. None of that applies to what a physician group signs.
For a provider, four families of value-based care contracts cover nearly every real proposal:
- Pay for performance (P4P). Fee-for-service claims continue as normal. The payer adds a quality-bonus overlay of financial incentives for hitting defined measures. Downside risk is zero. Operational lift is mostly reporting.
- Shared savings. A total-cost-of-care (TCOC) benchmark is set for an attributed population. If actual spend comes in under the benchmark and quality gates are met, the group shares in the savings. Upside-only arrangements carry no downside. Two-sided arrangements also share losses when spend exceeds the benchmark.
- Capitation and delegated risk. The payer pays a per-member-per-month (PMPM) amount to cover services rendered (or a defined subset) for an attributed panel. Common in Medicare Advantage and Medicaid managed care. The group takes on direct underwriting risk.
- Bundled or episode-based payments. One payment covers a defined episode of care (oncology, maternity, or a knee replacement). Mostly specialty. Risk is concentrated on a single episode rather than a population.
Every recommendation in this playbook refers to provider VBCs only. Knowing which family you are being offered is the first filter. Whether your group can actually operate it is the second.
The physician group readiness test: can you operate a value-based contract?
A physician group is ready to sign a value-based contract when it passes at least five of six readiness dimensions: claims data feeds, attribution transparency, care-management capacity, risk-adjustment capability, quality-reporting infrastructure, and an 18-month cash-flow cushion. Work through each dimension before the contract goes to outside counsel. A proposal that fails three or more dimensions is a group-readiness problem first and a contract problem second.
- Claims data feeds. Does the payer commit in writing to monthly claims or attribution files delivered within 45 days of the service month? Without reliable contract data feeding your analytics and internal data systems, the group is flying blind until year-end reconciliation. Ask for the file format, the fields included, and the delivery SLA as a contract exhibit, not a verbal assurance.
- Attribution transparency. Can your analytics team reproduce the payer's attribution methodology on a sample month using your existing data sources? Prospective attribution (assigned at the start of the year) and retrospective attribution (assigned after claims run out) produce very different patient panels. If the payer will not publish the exact logic, the attributed list is unauditable.
- Care-management capacity. A working ratio is one full-time care manager per 2,500 to 5,000 attributed lives, depending on population acuity. A high-acuity Medicare Advantage panel pushes the ratio tighter. Care coordination incentivizes quality improvement across avoidable hospitalization and readmission rates, and groups incentivized by shared savings compete directly on those two numbers. If the group has zero care managers and the proposal assumes active care management, the patient outcomes the contract rewards are unreachable.
- Risk-adjustment capability. HCC coding workflows directly change the benchmark in Medicare Advantage and ACO contracts. A group without annual wellness-visit workflows, chart-prep tooling, and coder auditing leaves risk adjustment on the table and receives a benchmark that understates patient complexity.
- Quality-reporting infrastructure. Sherri Onyiego, MD, PhD, FAAFP, Medical Director at Equality Health, described the operational reality in Physicians Practice: "Seven APM contracts with different health plans typically means seven sets of metrics. Practice staff must go to different portals, because each plan has their own way to submit information, communicate, and share performance reports." If your group cannot consolidate quality measurement across payers, the measure set in any new contract becomes marginal lift on an already-saturated team.
- Financial cushion. Dr. Onyiego again: "Traditionally, payment is at the end of the performance year. If the performance year is a calendar year, that could mean waiting 18 to 20 months to get a check." Run the 18-month cash-flow scenario before the contract is signed. If the group cannot absorb the lag, upside-only P4P or a capitated PMPM model with monthly cash flow is a safer entry point than two-sided shared savings.
A group that passes five or six dimensions is ready to negotiate terms. A group that fails two or more should treat the readiness gap as the first project, and the contract as the second.
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
What "market-standard" value-based contract terms look like
Market-standard value-based contract terms vary by arrangement type, but a physician group can benchmark any proposal against five levers: shared-savings split, minimum savings rate or minimum loss rate (MSR and MLR), quality-bonus pool size, PMPM adequacy, and benchmark methodology. Each lever has a direct financial impact on year-end reconciliation. Payers rarely volunteer the ranges below. Once you know them, every negotiation shifts.

Shared-savings split. In upside-only arrangements, 50/50 is a defensible starting point, and well-prepared groups with strong data availability and measurable savings track records push to 60/40 in their favor. In two-sided arrangements with real downside, the group's share should climb with the risk taken. Expect 70/30 or better if the group is taking on two-sided risk with a symmetric loss share. Anything under 50% for the group in a two-sided deal is a payer-leaning term.
Minimum savings rate and minimum loss rate. The MSR is the threshold the group must beat before savings become payable. MSRs wider than 3% materially erase smaller panels' savings because random variance alone can consume the margin. According to CMS's Medicare Shared Savings Program financial methodology, the MSR sliding scale tightens as the attributed population grows. Apply the same logic to commercial plans: smaller panels should have tighter thresholds that represent meaningful performance, not wider ones.
Quality-bonus pool size. For P4P overlays, a bonus pool below 2% of professional-fee revenue rarely covers the reporting cost. Bonus pools of 4% to 10% are in the range where the administrative lift pays off. A workable pool defines the measurement of each outcome measure, identifies a set of outcomes contingent upon care delivered, and sets thresholds that represent better outcomes rather than activity. If the pool is quoted as a percentage of total cost of care, convert it back to a percentage of your professional-fee revenue before comparing, and quantify how much of the bonus actually reaches clinical outcomes the group can influence.
PMPM adequacy for delegated capitation. A PMPM is only as good as the services it covers and the population risk it assumes. Compare the offered PMPM against published Medicare Advantage bid data, Milliman actuarial benchmarks, and the risk-adjusted equivalent under your group's current fee-for-service book. A PMPM that looks generous on a raw basis can fall short once delegation costs (care management, utilization management, auditing and adjudication support) are loaded in. The goal is a cost-effective capitation rate that is mutually recognized by both parties as acceptable to both parties and sustainable over the contract terms.
Benchmark methodology and rebasing. Historical benchmarks reward groups with a high baseline spend. Regional benchmarks reward efficient groups by comparing against peers. Blended benchmarks do both. The rebase rule matters more than the initial benchmark: a contract that rebases the benchmark to last year's performance punishes improvement by making each year's target harder. Ask the payer to show three consecutive years of rebasing math, publicly disclosed where possible, before you accept the methodology.
Benchmarks give you the numbers to push back on. The next step is reading the contract for the clauses that quietly shift risk onto the group.
Red flags in a value-based contract: seven clauses to strike, renegotiate, or walk away from
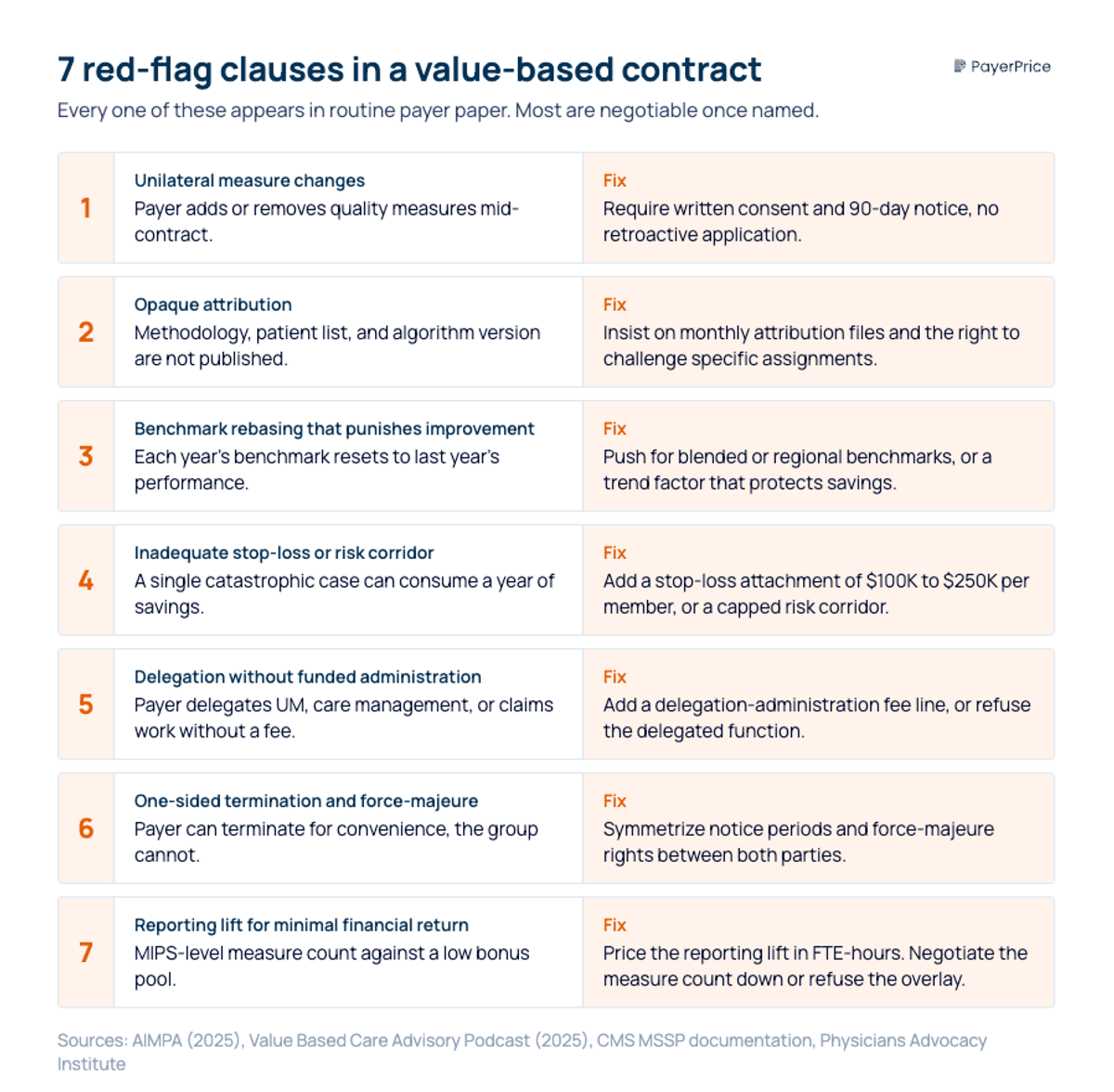
Seven clauses should prompt a physician group to strike, renegotiate, or walk away from a value-based contract: unilateral measure changes, opaque attribution, benchmark rebasing that punishes improvement, inadequate stop-loss, delegation without funded administration, one-sided termination, and heavy reporting lift for minimal financial return. Each one appears in routine payer paper. Most are negotiable once named, and naming them early helps mitigate the unintended consequences of a rushed signature.
1. Unilateral measure changes
The payer reserves the right to add, remove, or modify quality metrics mid-contract. A group signs to 12 measures, operationalizes 12 measures, and finds 18 measures in the Q3 performance report. Replace with a change-control clause: measure changes require written consent and a 90-day notice, with no retroactive application.
2. Opaque or one-sided attribution
The contract names an attribution methodology but does not bind the payer to publish the logic, the patient list, or the algorithm version. Without audit rights on attribution, the group cannot dispute a patient who was assigned to its panel for cost purposes but never walked in the door. Insist on monthly attribution files, a documented methodology, and the right to challenge specific assignments.
3. Benchmark rebasing that punishes improvement
The benchmark resets each year to the group's prior-year performance, so every dollar of savings makes next year's target harder. Over three years, an improving group reaches a floor where no further savings are possible. Push for blended or regional benchmarks, or for a rebase trend factor that protects a portion of improvement.
4. Inadequate or missing stop-loss and risk corridor
In two-sided risk and capitation, a single catastrophic case can consume a year of savings. The contract should include stop-loss at a per-member attachment point appropriate to the population (for most commercial panels, $100,000 to $250,000 per member per year) or a risk corridor that caps downside exposure. No stop-loss plus no corridor equals uncapped tail risk and unpredictable out-of-pocket losses on high-cost cases.
5. Delegation without funded administration
Medicare Advantage plans increasingly push delegation of utilization management, care management, and claims functions to provider groups. Alex Yarijanian, host of the Value Based Care Advisory Podcast, put the 2026 trend plainly: "Delegation is no longer a reward. It's a stress test. I'm seeing delegation agreements where plans are not even paying providers for the delegated functions, meaning more operational burden, more audit exposure, more downside, with no proportional upside." If the payer wants delegation, the payer funds delegation. Add a delegation-administration fee line or refuse the delegated function.
6. One-sided termination and force-majeure
The payer can terminate for convenience in 60 days, the group cannot. The payer's force-majeure rights suspend payment obligations, the group's rights do not. Symmetrize both clauses. Neither party should be able to walk without the same notice the other party must give.
7. MIPS-level reporting lift for minimal financial return
David Eagle, MD, President of the American Independent Medical Practice Association (AIMPA), captured the economics of low-reward reporting: "Meeting MIPS requirements is a big deal, and it's hard, and there's really not much reward for that." Before signing, quantify the reporting lift in FTE-hours and compare it against the total bonus pool. If the math does not clear the lift, negotiate down the measure count or refuse the quality overlay.
A contract that strikes all seven red flags is close to signable. The final check is putting the payer on record for the mechanics they did not write down.
10 questions to ask a payer before signing a value-based care contract
These ten questions force the payer to document attribution, benchmarking, data cadence, stop-loss, downside corridors, measure rationale, audit rights, claims-feed timing, termination, and dispute resolution in writing before the contract is final. Send them in an email, request written responses, and file the replies as a contract exhibit.
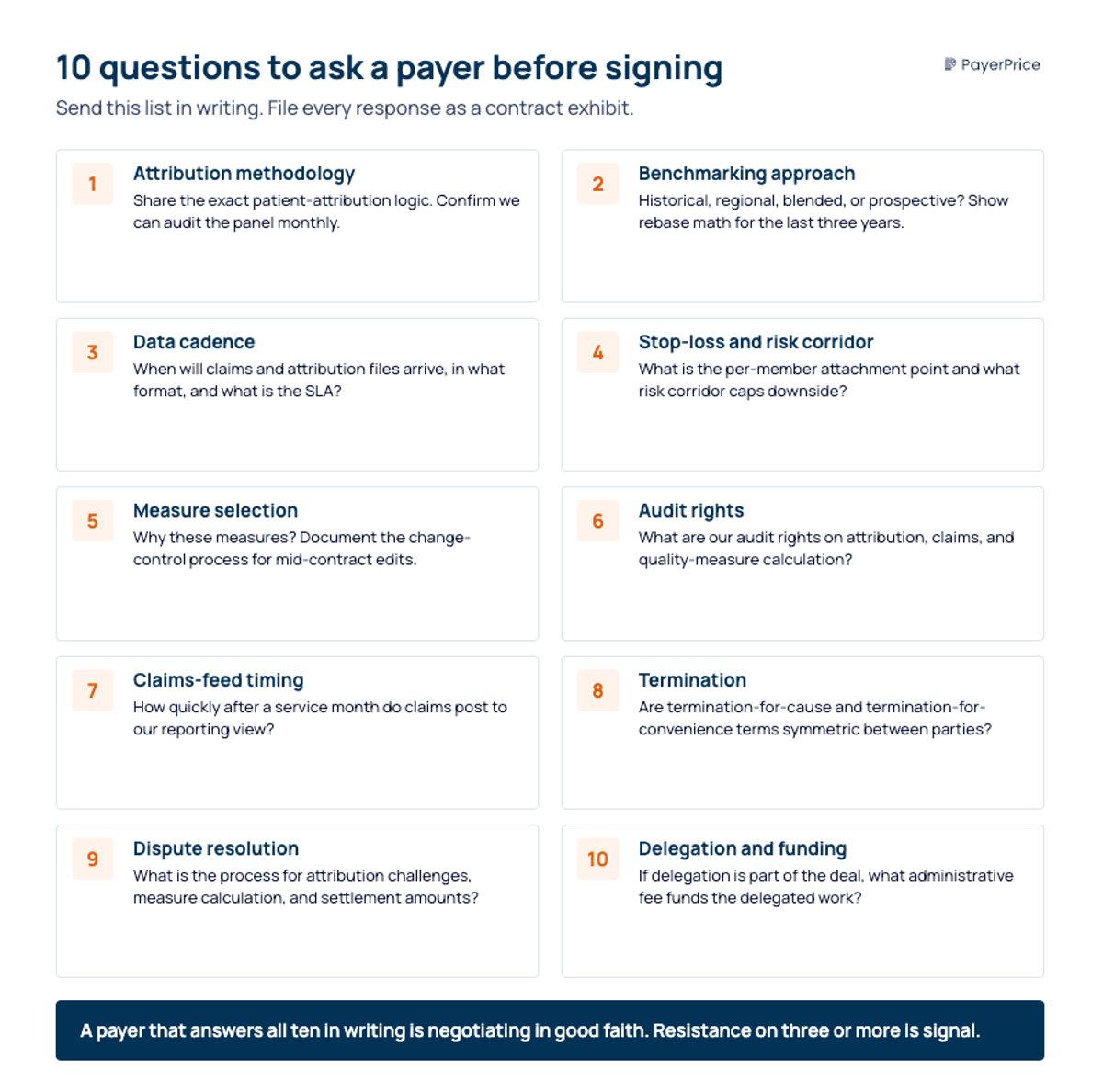
- Attribution methodology. What is the exact patient-attribution logic, and can we audit the attributed panel monthly?
- Benchmarking approach. Is the benchmark historical, regional, blended, or prospective? Show the rebasing math for the last three years.
- Data cadence. When will we receive claims and attribution files, in what format, and what is the SLA?
- Stop-loss and risk corridor. What is the per-member attachment point for stop-loss, and what risk corridor caps downside?
- Measure selection rationale. Why these measures, what is the change-control process for modifying them mid-contract, and does the pool reimburse adherence and clinical or economic benefits rather than volume?
- Audit rights. What are our audit rights on attribution, claims, and quality-measure calculation?
- Claims-feed timing. How quickly after a service month will claims post to our reporting view?
- Termination. What are the termination-for-cause and termination-for-convenience terms, and are they symmetric between payer and group?
- Dispute resolution. What is the dispute-resolution process for attribution challenges, measure calculation, and settlement amounts?
- Delegated functions and funding. If delegation is part of the deal, what administrative fee funds the delegated work?
A payer that answers all ten in writing is negotiating in good faith. A payer that resists three or more is telling you something about the contract you should believe.
Should you sign? A decision framework
The three parts of this playbook converge on a simple decision heuristic.
Sign when your group passes five or six readiness dimensions, the proposed terms land inside the benchmark ranges above, and no red-flag clauses remain in the final document. A deal that clears all three gates is a real value-based contract with patient-centered incentives, not a risk transfer disguised as one.
Negotiate, do not reject when readiness is partial and the payer will move on terms. The most common version of this path is an upside-only P4P first year, a two-sided year two contingent on a readiness milestone, and a renegotiation of any red-flag clause before either party countersigns.
Walk away or delay when the downside exposure outpaces your readiness, or when two or more red-flag clauses cannot be struck. Walking away from a bad contract protects next year's negotiating position more than signing a marginal one ever will.
The fastest concrete step you can take today: pull the proposal currently on your desk, run the six-dimension readiness test against it, and mark every clause that matches the seven red flags. That document becomes the agenda for your next payer meeting, and the evidence base for every term you change before you sign.
Share this article
Help spread the knowledge by sharing with others
Ready to see how your rates compare?
PayerPrice gives you instant access to negotiated rate data across payers and providers so you can benchmark, negotiate, and optimize with confidence.
Related Articles
Continue exploring healthcare transparency and compliance topics
How to Model a Payer Contract: A Provider's Guide
See how providers model payer contracts against real claims to catch a money-losing deal before signing. Formulas, a worked example, and a 5-step method.
How to Run Payer Contract Analytics (Physician Group Guide)
Stop signing stealth pay cuts. This guide shows physician groups how to benchmark rates, recover underpayments, and run payer contract analytics in-house.
How to Contract With Insurance Companies (Without a Bad Rate)
How to contract with insurance companies as a provider: the credentialing steps, the contract clauses to check, and how to tell if your rate is fair before you sign.